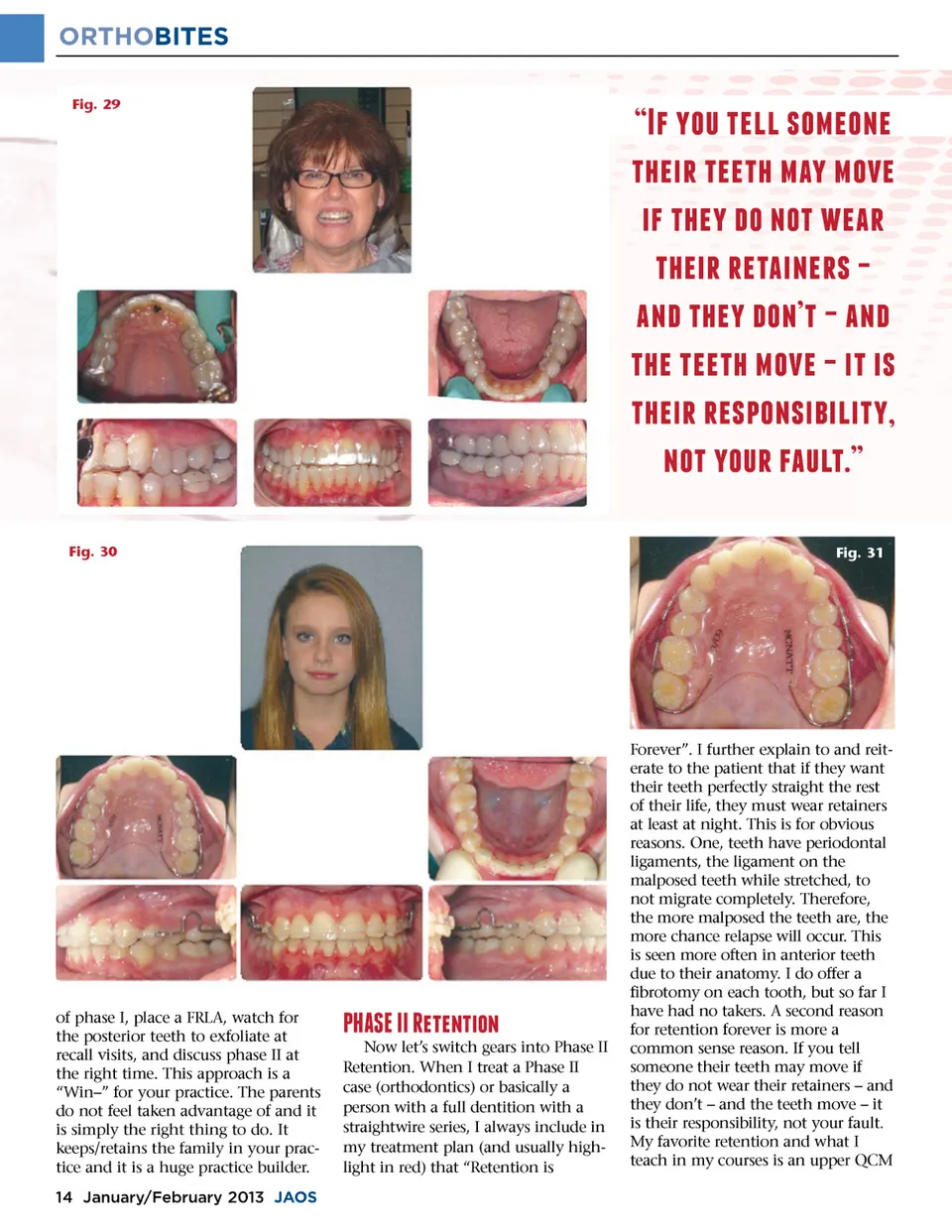
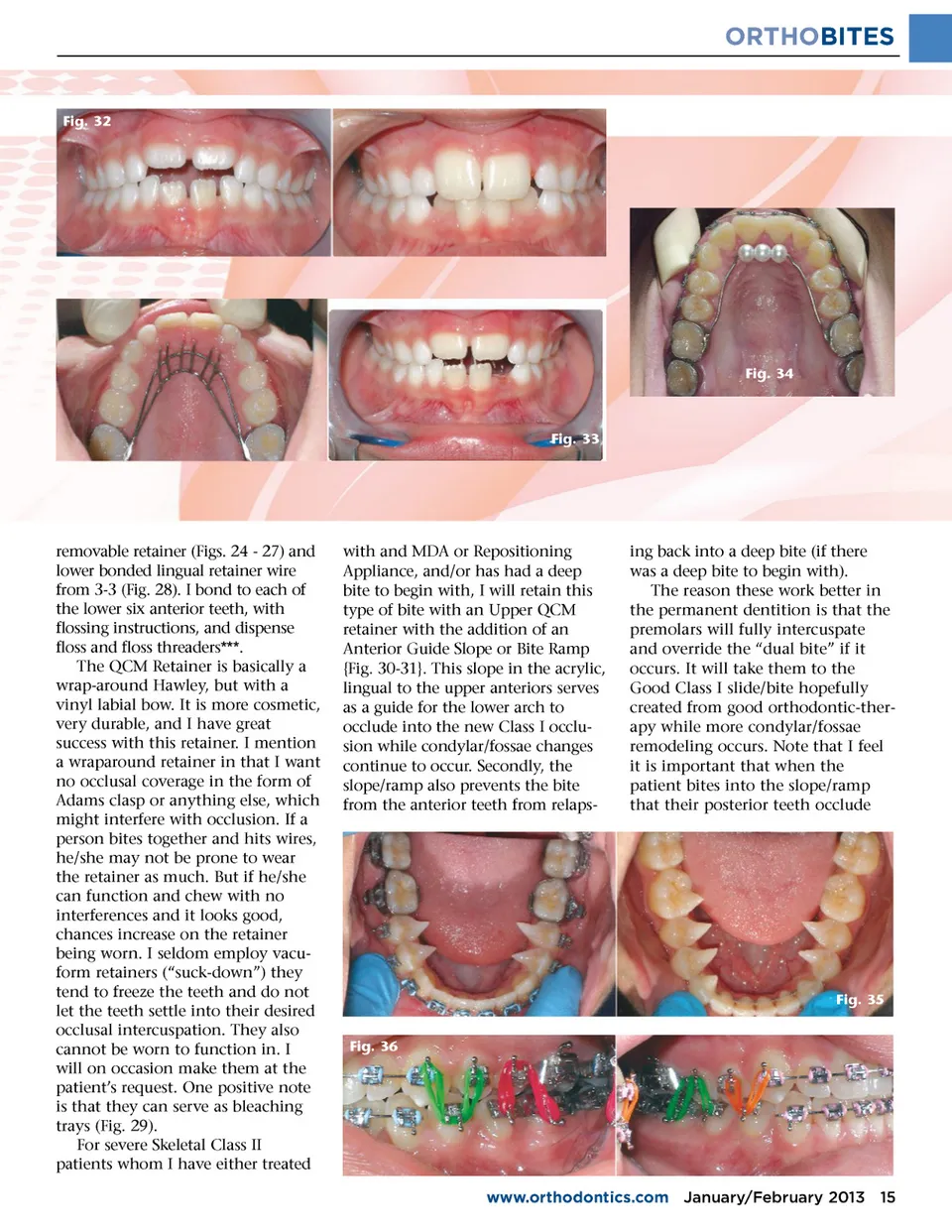
ORTHOBITES Fig. 32 Fig. 34 Fig. 33 removable retainer (Figs. 24 -27) and lower bonded lingual retainer wire from 3-3 (Fig. 28). I bond to each of the lower six anterior teeth, with flossing instructions, and dispense floss and floss threaders***. The QCM Retainer is basically a wrap-around Hawley, but with a vinyl labial bow. It is more cosmetic, very durable, and I have great success with this retainer. I mention a wraparound retainer in that I want no occlusal coverage in the form of Adams clasp or anything else, which might interfere with occlusion. If a person bites together and hits wires, he/she may not be prone to wear the retainer as much. But if he/she can function and chew with no interferences and it looks good, chances increase on the retainer being worn. I seldom employ vacu-form retainers (“suck-down”) they tend to freeze the teeth and do not let the teeth settle into their desired occlusal intercuspation. They also cannot be worn to function in. I will on occasion make them at the patient’s request. One positive note is that they can serve as bleaching trays (Fig. 29). For severe Skeletal Class II patients whom I have either treated with and MDA or Repositioning Appliance, and/or has had a deep bite to begin with, I will retain this type of bite with an Upper QCM retainer with the addition of an Anterior Guide Slope or Bite Ramp {Fig. 30-31}. This slope in the acrylic, lingual to the upper anteriors serves as a guide for the lower arch to occlude into the new Class I occlu-sion while condylar/fossae changes continue to occur. Secondly, the slope/ramp also prevents the bite from the anterior teeth from relaps-ing back into a deep bite (if there was a deep bite to begin with). The reason these work better in the permanent dentition is that the premolars will fully intercuspate and override the “dual bite” if it occurs. It will take them to the Good Class I slide/bite hopefully created from good orthodontic-ther-apy while more condylar/fossae remodeling occurs. Note that I feel it is important that when the patient bites into the slope/ramp that their posterior teeth occlude Fig. 35 Fig. 36 www.orthodontics.com January/February 2013 15
Journal of the American Orthodontic Society January-February 2013: Page 15