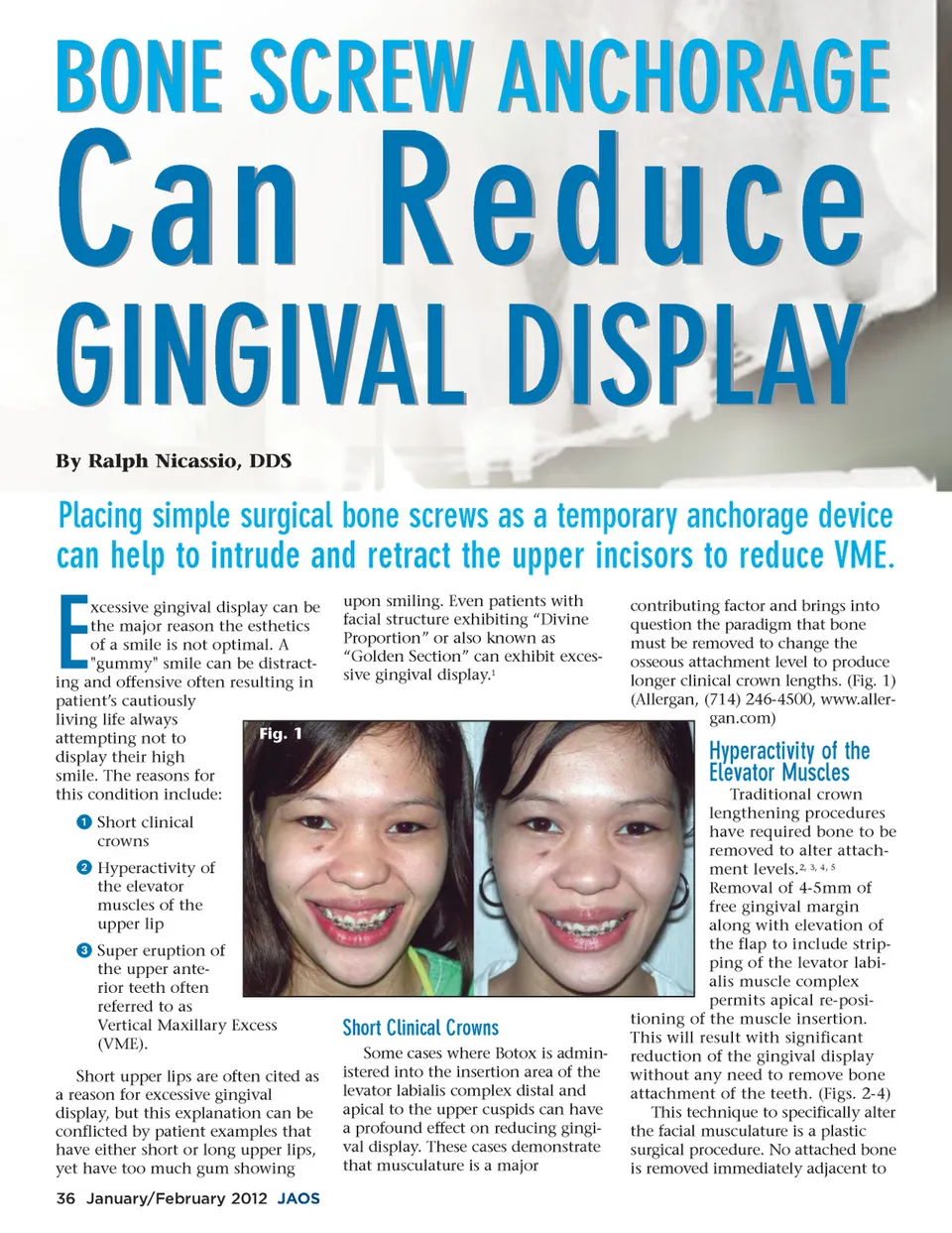
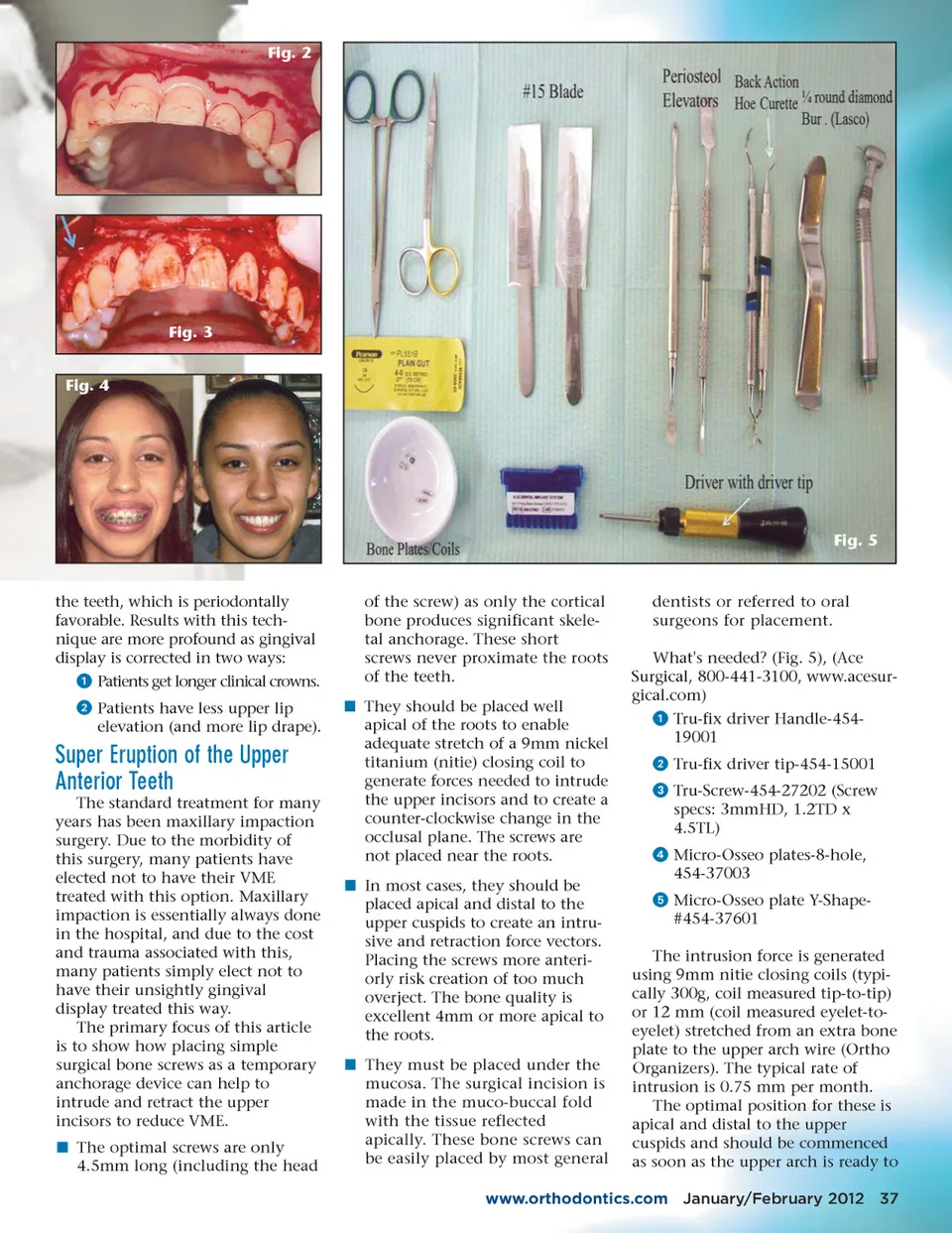
Fig. 2 Fig. 3 Fig. 4 Fig. 5 the teeth, which is periodontally favorable. Results with this tech-nique are more profound as gingival display is corrected in two ways: ᕡ Patients get longer clinical crowns. ᕢ Patients have less upper lip elevation (and more lip drape). of the screw) as only the cortical bone produces significant skele-tal anchorage. These short screws never proximate the roots of the teeth. í They should be placed well apical of the roots to enable adequate stretch of a 9mm nickel titanium (nitie) closing coil to generate forces needed to intrude the upper incisors and to create a counter-clockwise change in the occlusal plane. The screws are not placed near the roots. í In most cases, they should be placed apical and distal to the upper cuspids to create an intru-sive and retraction force vectors. Placing the screws more anteri-orly risk creation of too much overject. The bone quality is excellent 4mm or more apical to the roots. í They must be placed under the mucosa. The surgical incision is made in the muco-buccal fold with the tissue reflected apically. These bone screws can be easily placed by most general dentists or referred to oral surgeons for placement. What's needed? (Fig. 5), (Ace Surgical, 800-441-3100, www.acesur-gical.com) ᕡ Tru-fix driver Handle-454-19001 ᕢ Tru-fix driver tip-454-15001 ᕣ Tru-Screw-454-27202 (Screw specs: 3mmHD, 1.2TD x 4.5TL) ᕤ Micro-Osseo plates-8-hole, 454-37003 ᕥ Micro-Osseo plate Y-Shape-#454-37601 The intrusion force is generated using 9mm nitie closing coils (typi-cally 300g, coil measured tip-to-tip) or 12 mm (coil measured eyelet-to-eyelet) stretched from an extra bone plate to the upper arch wire (Ortho Organizers). The typical rate of intrusion is 0.75 mm per month. The optimal position for these is apical and distal to the upper cuspids and should be commenced as soon as the upper arch is ready to Super Eruption of the Upper Anterior Teeth The standard treatment for many years has been maxillary impaction surgery. Due to the morbidity of this surgery, many patients have elected not to have their VME treated with this option. Maxillary impaction is essentially always done in the hospital, and due to the cost and trauma associated with this, many patients simply elect not to have their unsightly gingival display treated this way. The primary focus of this article is to show how placing simple surgical bone screws as a temporary anchorage device can help to intrude and retract the upper incisors to reduce VME. í The optimal screws are only 4.5mm long (including the head www.orthodontics.com January/February 2012 37
Journal of the American Orthodontic Society January-February 2012: Page 37