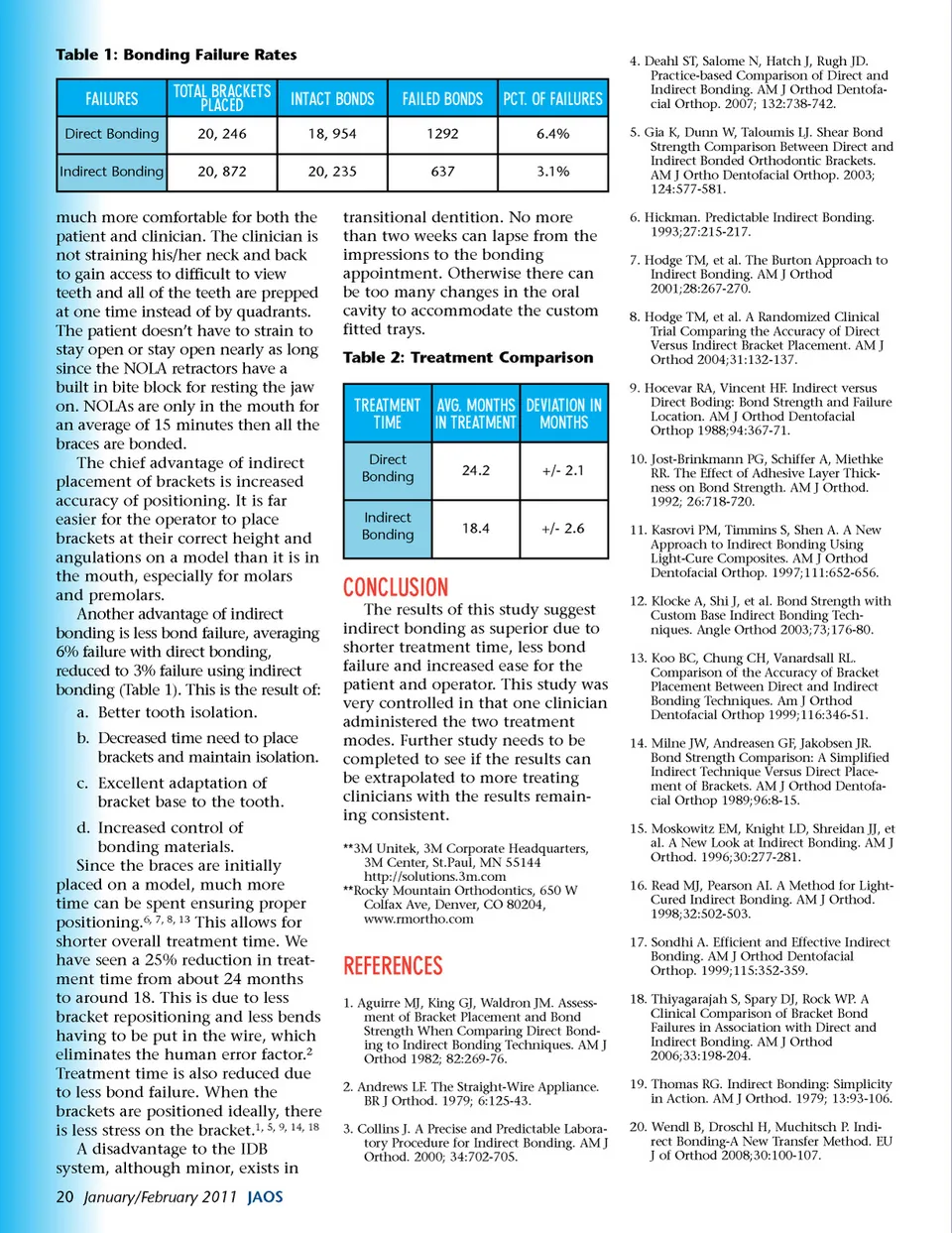
Table 1: Bonding Failure Rates FAILURES Direct Bonding Indirect Bonding TOTAL BRACKETS PLACED 20, 246 20, 872 INTACT BONDS 18, 954 20, 235 FAILED BONDS 1292 637 PCT. OF FAILURES 6.4% 3.1% 4. Deahl ST, Salome N, Hatch J, Rugh JD. Practice-based Comparison of Direct and Indirect Bonding. AM J Orthod Dentofa-cial Orthop. 2007; 132:738-742. 5. Gia K, Dunn W, Taloumis LJ. Shear Bond Strength Comparison Between Direct and Indirect Bonded Orthodontic Brackets. AM J Ortho Dentofacial Orthop. 2003; 124:577-581. 6. Hickman. Predictable Indirect Bonding. 1993;27:215-217. 7. Hodge TM, et al. The Burton Approach to Indirect Bonding. AM J Orthod 2001;28:267-270. 8. Hodge TM, et al. A Randomized Clinical Trial Comparing the Accuracy of Direct Versus Indirect Bracket Placement. AM J Orthod 2004;31:132-137. 9. Hocevar RA, Vincent HF. Indirect versus Direct Boding: Bond Strength and Failure Location. AM J Orthod Dentofacial Orthop 1988;94:367-71. 10. Jost-Brinkmann PG, Schiffer A, Miethke RR. The Effect of Adhesive Layer Thick-ness on Bond Strength. AM J Orthod. 1992; 26:718-720. 11. Kasrovi PM, Timmins S, Shen A. A New Approach to Indirect Bonding Using Light-Cure Composites. AM J Orthod Dentofacial Orthop. 1997;111:652-656. 12. Klocke A, Shi J, et al. Bond Strength with Custom Base Indirect Bonding Tech-niques. Angle Orthod 2003;73;176-80. 13. Koo BC, Chung CH, Vanardsall RL. Comparison of the Accuracy of Bracket Placement Between Direct and Indirect Bonding Techniques. Am J Orthod Dentofacial Orthop 1999;116:346-51. 14. Milne JW, Andreasen GF, Jakobsen JR. Bond Strength Comparison: A Simplified Indirect Technique Versus Direct Place-ment of Brackets. AM J Orthod Dentofa-cial Orthop 1989;96:8-15. 15. Moskowitz EM, Knight LD, Shreidan JJ, et al. A New Look at Indirect Bonding. AM J Orthod. 1996;30:277-281. 16. Read MJ, Pearson AI. A Method for Light-Cured Indirect Bonding. AM J Orthod. 1998;32:502-503. 17. Sondhi A. Efficient and Effective Indirect Bonding. AM J Orthod Dentofacial Orthop. 1999;115:352-359. 18. Thiyagarajah S, Spary DJ, Rock WP. A Clinical Comparison of Bracket Bond Failures in Association with Direct and Indirect Bonding. AM J Orthod 2006;33:198-204. 19. Thomas RG. Indirect Bonding: Simplicity in Action. AM J Orthod. 1979; 13:93-106. 20. Wendl B, Droschl H, Muchitsch P. Indi-rect Bonding-A New Transfer Method. EU J of Orthod 2008;30:100-107. much more comfortable for both the patient and clinician. The clinician is not straining his/her neck and back to gain access to difficult to view teeth and all of the teeth are prepped at one time instead of by quadrants. The patient doesn’t have to strain to stay open or stay open nearly as long since the NOLA retractors have a built in bite block for resting the jaw on. NOLAs are only in the mouth for an average of 15 minutes then all the braces are bonded. The chief advantage of indirect placement of brackets is increased accuracy of positioning. It is far easier for the operator to place brackets at their correct height and angulations on a model than it is in the mouth, especially for molars and premolars. Another advantage of indirect bonding is less bond failure, averaging 6% failure with direct bonding, reduced to 3% failure using indirect bonding (Table 1). This is the result of: a. Better tooth isolation. b. Decreased time need to place brackets and maintain isolation. c. Excellent adaptation of bracket base to the tooth. d. Increased control of bonding materials. Since the braces are initially placed on a model, much more time can be spent ensuring proper positioning. 6, 7, 8, 13 This allows for shorter overall treatment time. We have seen a 25% reduction in treat-ment time from about 24 months to around 18. This is due to less bracket repositioning and less bends having to be put in the wire, which eliminates the human error factor. 2 Treatment time is also reduced due to less bond failure. When the brackets are positioned ideally, there is less stress on the bracket. 1, 5, 9, 14, 18 A disadvantage to the IDB system, although minor, exists in 20 January/February 2011 JAOS transitional dentition. No more than two weeks can lapse from the impressions to the bonding appointment. Otherwise there can be too many changes in the oral cavity to accommodate the custom fitted trays. Table 2: Treatment Comparison TREATMENT AVG. MONTHS DEVIATION IN TIME IN TREATMENT MONTHS Direct Bonding Indirect Bonding 24.2 +/-2.1 18.4 +/-2.6 CONCLUSION The results of this study suggest indirect bonding as superior due to shorter treatment time, less bond failure and increased ease for the patient and operator. This study was very controlled in that one clinician administered the two treatment modes. Further study needs to be completed to see if the results can be extrapolated to more treating clinicians with the results remain-ing consistent. **3M Unitek, 3M Corporate Headquarters, 3M Center, St.Paul, MN 55144 http://solutions.3m.com **Rocky Mountain Orthodontics, 650 W Colfax Ave, Denver, CO 80204, www.rmortho.com REFERENCES 1. Aguirre MJ, King GJ, Waldron JM. Assess-ment of Bracket Placement and Bond Strength When Comparing Direct Bond-ing to Indirect Bonding Techniques. AM J Orthod 1982; 82:269-76. 2. Andrews LF. The Straight-Wire Appliance. BR J Orthod. 1979; 6:125-43. 3. Collins J. A Precise and Predictable Labora-tory Procedure for Indirect Bonding. AM J Orthod. 2000; 34:702-705.
Journal of the American Orthodontic Society January - February 2011: Page 20