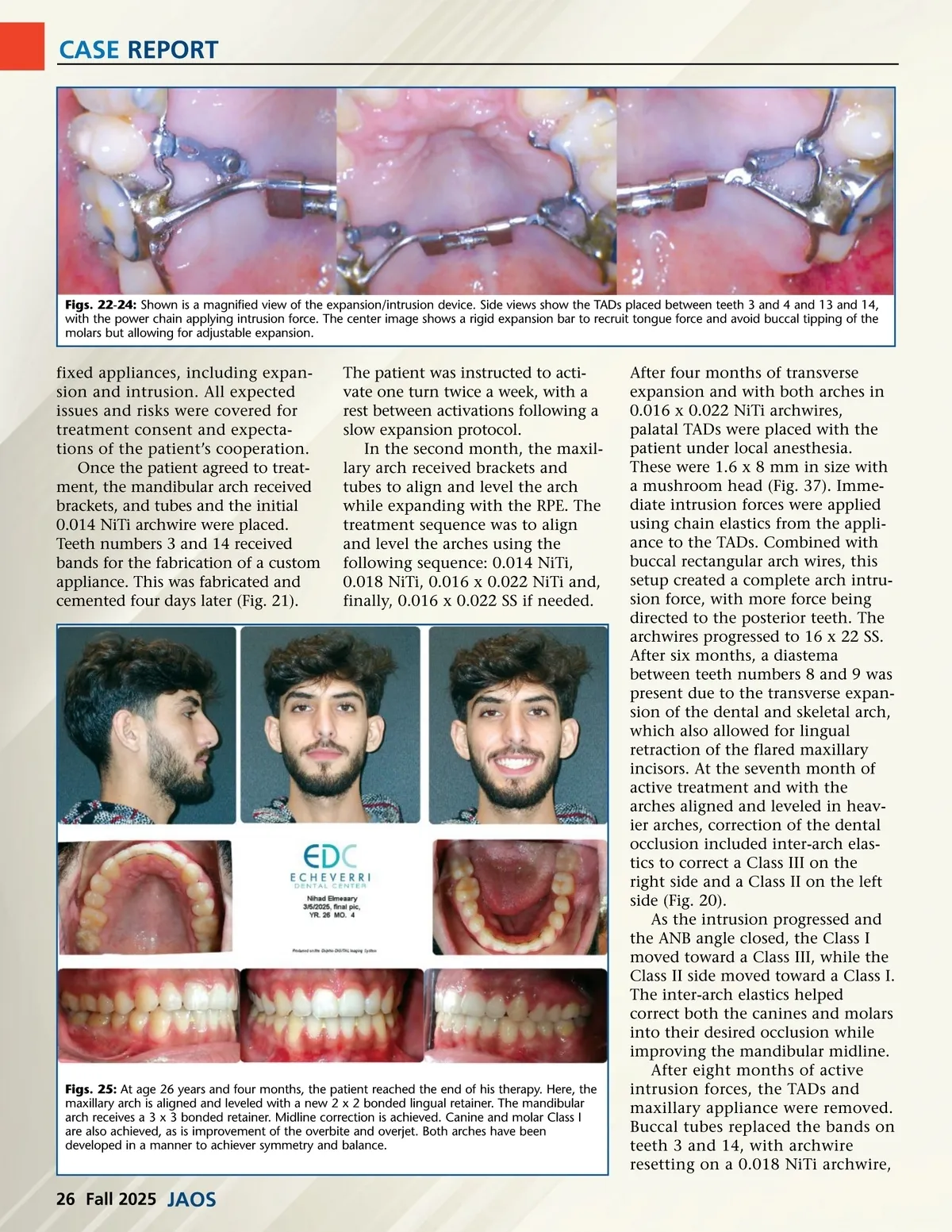
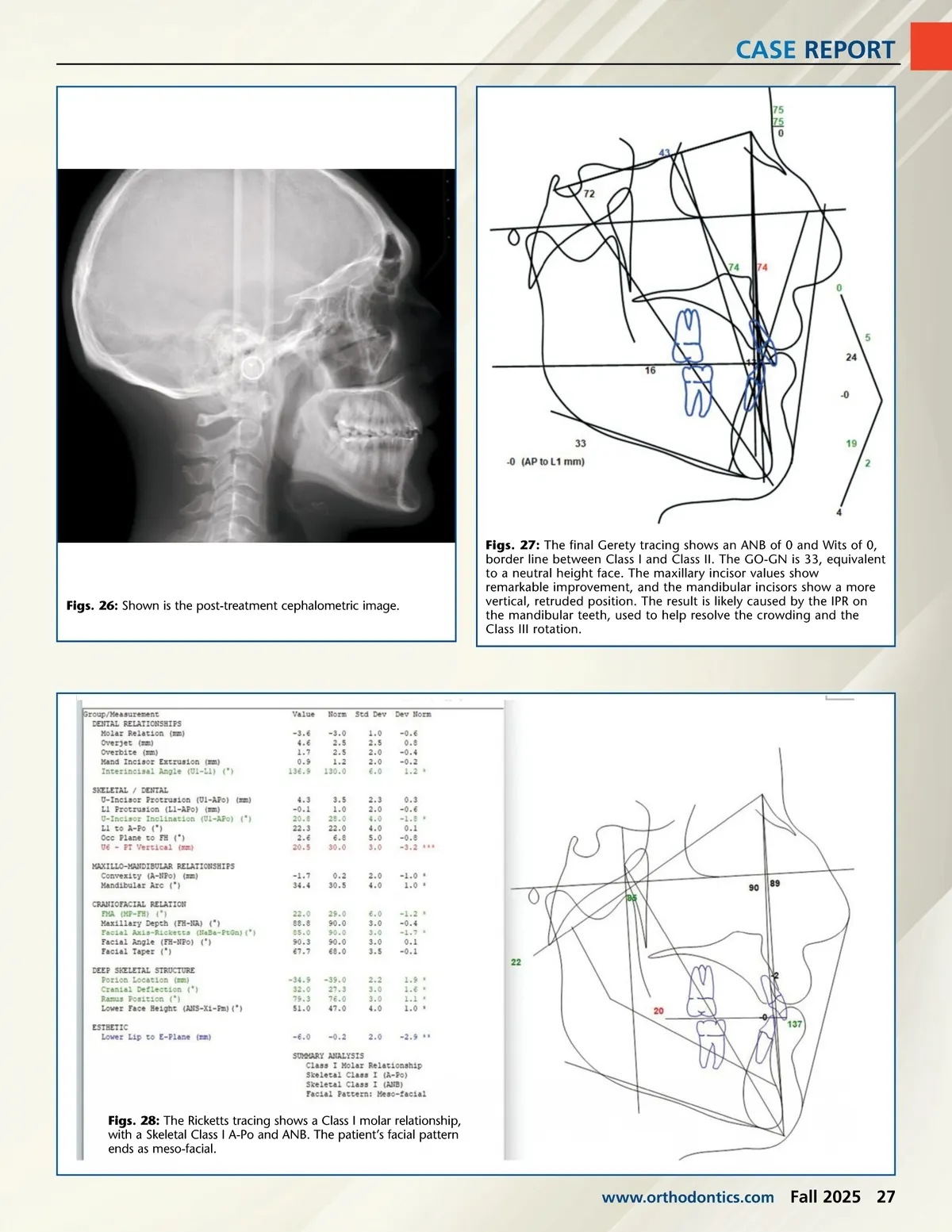
CASE REPORT Figs. 22-24: Shown is a magnified view of the expansion/intrusion device. Side views show the TADs placed between teeth 3 and 4 and 13 and 14, with the power chain applying intrusion force. The center image shows a rigid expansion bar to recruit tongue force and avoid buccal tipping of the molars but allowing for adjustable expansion. fixed appliances, including expan-sion and intrusion. All expected issues and risks were covered for treatment consent and expecta-tions of the patient’s cooperation. Once the patient agreed to treat-ment, the mandibular arch received brackets, and tubes and the initial 0.014 NiTi archwire were placed. Teeth numbers 3 and 14 received bands for the fabrication of a custom appliance. This was fabricated and cemented four days later (Fig. 21). The patient was instructed to acti-vate one turn twice a week, with a rest between activations following a slow expansion protocol. In the second month, the maxil-lary arch received brackets and tubes to align and level the arch while expanding with the RPE. The treatment sequence was to align and level the arches using the following sequence: 0.014 NiTi, 0.018 NiTi, 0.016 x 0.022 NiTi and, finally, 0.016 x 0.022 SS if needed. Figs. 25: At age 26 years and four months, the patient reached the end of his therapy. Here, the maxillary arch is aligned and leveled with a new 2 x 2 bonded lingual retainer. The mandibular arch receives a 3 x 3 bonded retainer. Midline correction is achieved. Canine and molar Class I are also achieved, as is improvement of the overbite and overjet. Both arches have been developed in a manner to achiever symmetry and balance. After four months of transverse expansion and with both arches in 0.016 x 0.022 NiTi archwires, palatal TADs were placed with the patient under local anesthesia. These were 1.6 x 8 mm in size with a mushroom head (Fig. 37). Imme-diate intrusion forces were applied using chain elastics from the appli-ance to the TADs. Combined with buccal rectangular arch wires, this setup created a complete arch intru-sion force, with more force being directed to the posterior teeth. The archwires progressed to 16 x 22 SS. After six months, a diastema between teeth numbers 8 and 9 was present due to the transverse expan-sion of the dental and skeletal arch, which also allowed for lingual retraction of the flared maxillary incisors. At the seventh month of active treatment and with the arches aligned and leveled in heav-ier arches, correction of the dental occlusion included inter-arch elas-tics to correct a Class III on the right side and a Class II on the left side (Fig. 20). As the intrusion progressed and the ANB angle closed, the Class I moved toward a Class III, while the Class II side moved toward a Class I. The inter-arch elastics helped correct both the canines and molars into their desired occlusion while improving the mandibular midline. After eight months of active intrusion forces, the TADs and maxillary appliance were removed. Buccal tubes replaced the bands on teeth 3 and 14, with archwire resetting on a 0.018 NiTi archwire, 26 Fall 2025 JAOS
Journal of the American Orthodontic Society Fall 2025: Page 26