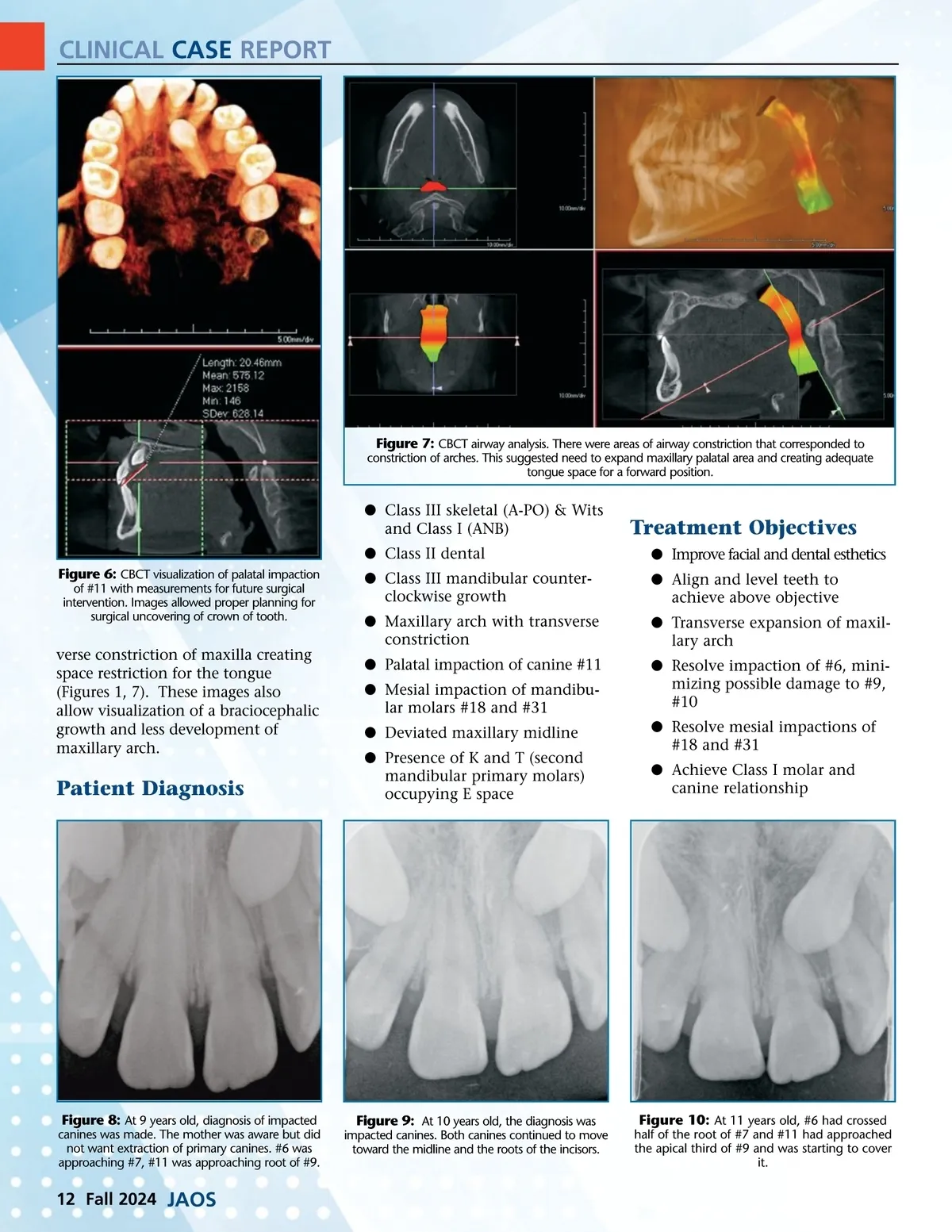
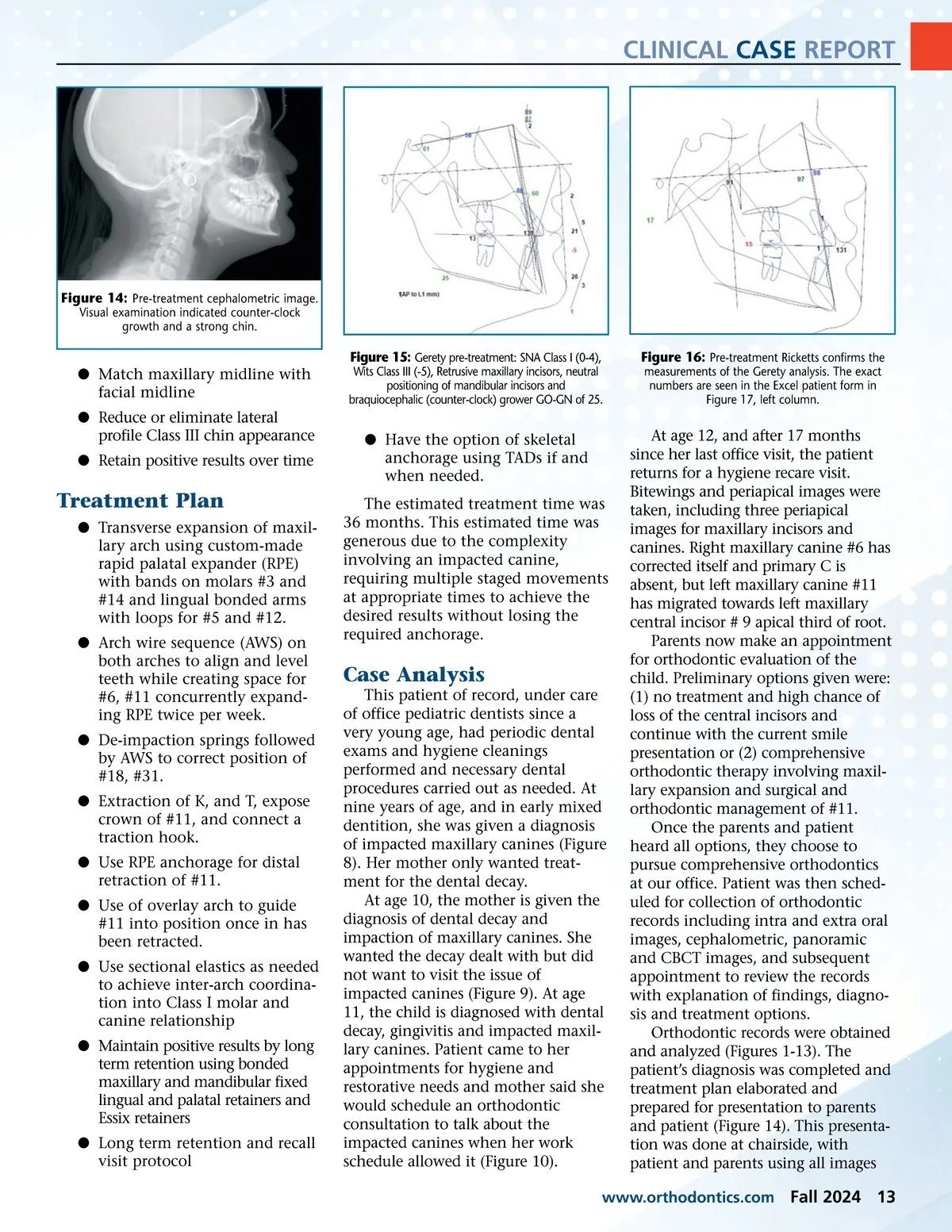
CLINICAL CASE REPORT Figure 14: Pre-treatment cephalometric image. Visual examination indicated counter-clock growth and a strong chin. b Match maxillary midline with facial midline b Reduce or eliminate lateral profile Class III chin appearance b Retain positive results over time Figure 15: Gerety pre-treatment: SNA Class I (0-4), Wits Class III (-5), Retrusive maxillary incisors, neutral positioning of mandibular incisors and braquiocephalic (counter-clock) grower GO-GN of 25. Figure 16: Pre-treatment Ricketts confirms the measurements of the Gerety analysis. The exact numbers are seen in the Excel patient form in Figure 17, left column. b Have the option of skeletal anchorage using TADs if and when needed. The estimated treatment time was 36 months. This estimated time was generous due to the complexity involving an impacted canine, requiring multiple staged movements at appropriate times to achieve the desired results without losing the required anchorage. Treatment Plan b Transverse expansion of maxil-lary arch using custom-made rapid palatal expander (RPE) with bands on molars #3 and #14 and lingual bonded arms with loops for #5 and #12. b Arch wire sequence (AWS) on both arches to align and level teeth while creating space for #6, #11 concurrently expand-ing RPE twice per week. b De-impaction springs followed by AWS to correct position of #18, #31. b Extraction of K, and T, expose crown of #11, and connect a traction hook. b Use RPE anchorage for distal retraction of #11. b Use of overlay arch to guide #11 into position once in has been retracted. b Use sectional elastics as needed to achieve inter-arch coordina-tion into Class I molar and canine relationship b Maintain positive results by long term retention using bonded maxillary and mandibular fixed lingual and palatal retainers and Essix retainers b Long term retention and recall visit protocol Case Analysis This patient of record, under care of office pediatric dentists since a very young age, had periodic dental exams and hygiene cleanings performed and necessary dental procedures carried out as needed. At nine years of age, and in early mixed dentition, she was given a diagnosis of impacted maxillary canines (Figure 8). Her mother only wanted treat-ment for the dental decay. At age 10, the mother is given the diagnosis of dental decay and impaction of maxillary canines. She wanted the decay dealt with but did not want to visit the issue of impacted canines (Figure 9). At age 11, the child is diagnosed with dental decay, gingivitis and impacted maxil-lary canines. Patient came to her appointments for hygiene and restorative needs and mother said she would schedule an orthodontic consultation to talk about the impacted canines when her work schedule allowed it (Figure 10). At age 12, and after 17 months since her last office visit, the patient returns for a hygiene recare visit. Bitewings and periapical images were taken, including three periapical images for maxillary incisors and canines. Right maxillary canine #6 has corrected itself and primary C is absent, but left maxillary canine #11 has migrated towards left maxillary central incisor # 9 apical third of root. Parents now make an appointment for orthodontic evaluation of the child. Preliminary options given were: (1) no treatment and high chance of loss of the central incisors and continue with the current smile presentation or (2) comprehensive orthodontic therapy involving maxil-lary expansion and surgical and orthodontic management of #11. Once the parents and patient heard all options, they choose to pursue comprehensive orthodontics at our office. Patient was then sched-uled for collection of orthodontic records including intra and extra oral images, cephalometric, panoramic and CBCT images, and subsequent appointment to review the records with explanation of findings, diagno-sis and treatment options. Orthodontic records were obtained and analyzed (Figures 1-13). The patient’s diagnosis was completed and treatment plan elaborated and prepared for presentation to parents and patient (Figure 14). This presenta-tion was done at chairside, with patient and parents using all images www.orthodontics.com Fall 2024 13
Journal of the American Orthodontic Society Fall 2024: Page 13