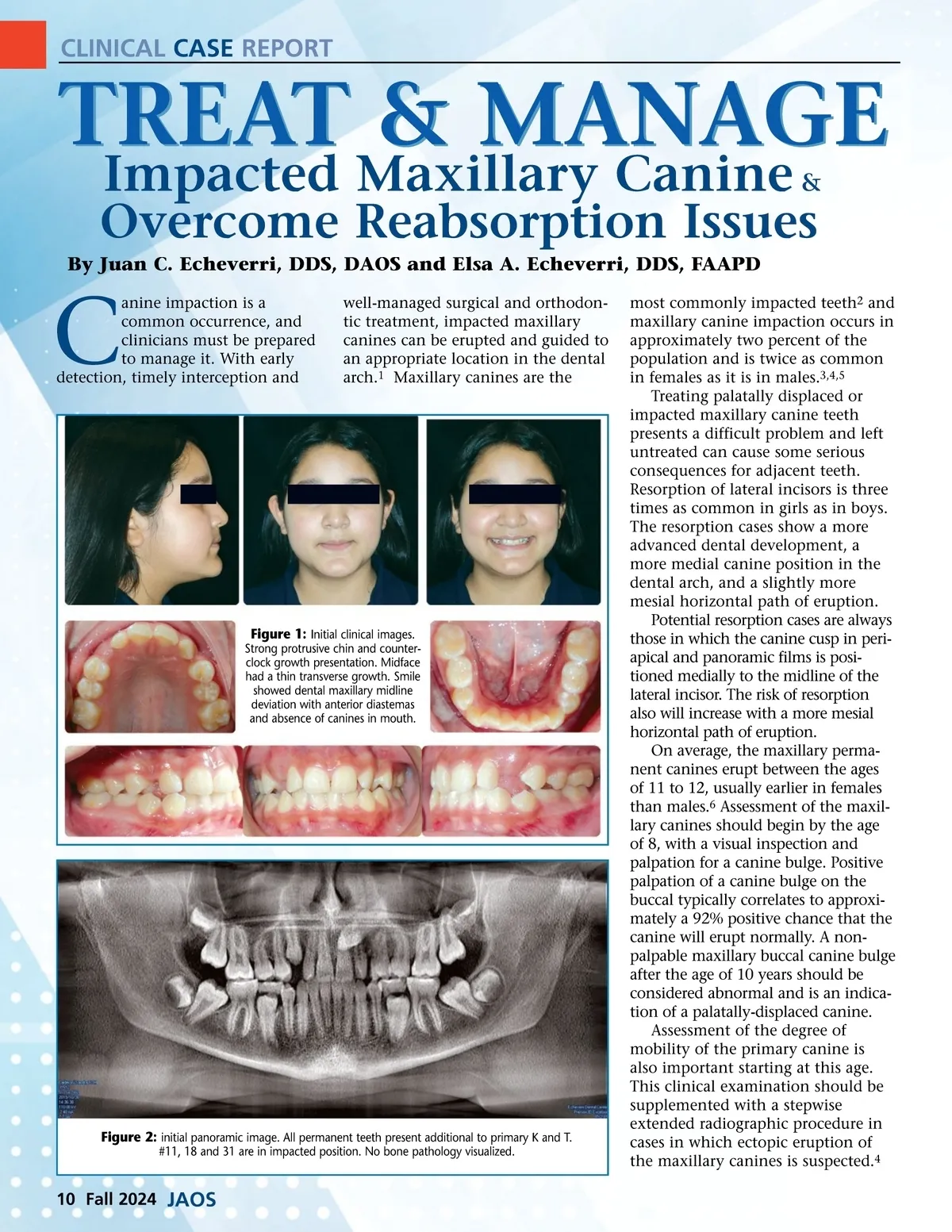
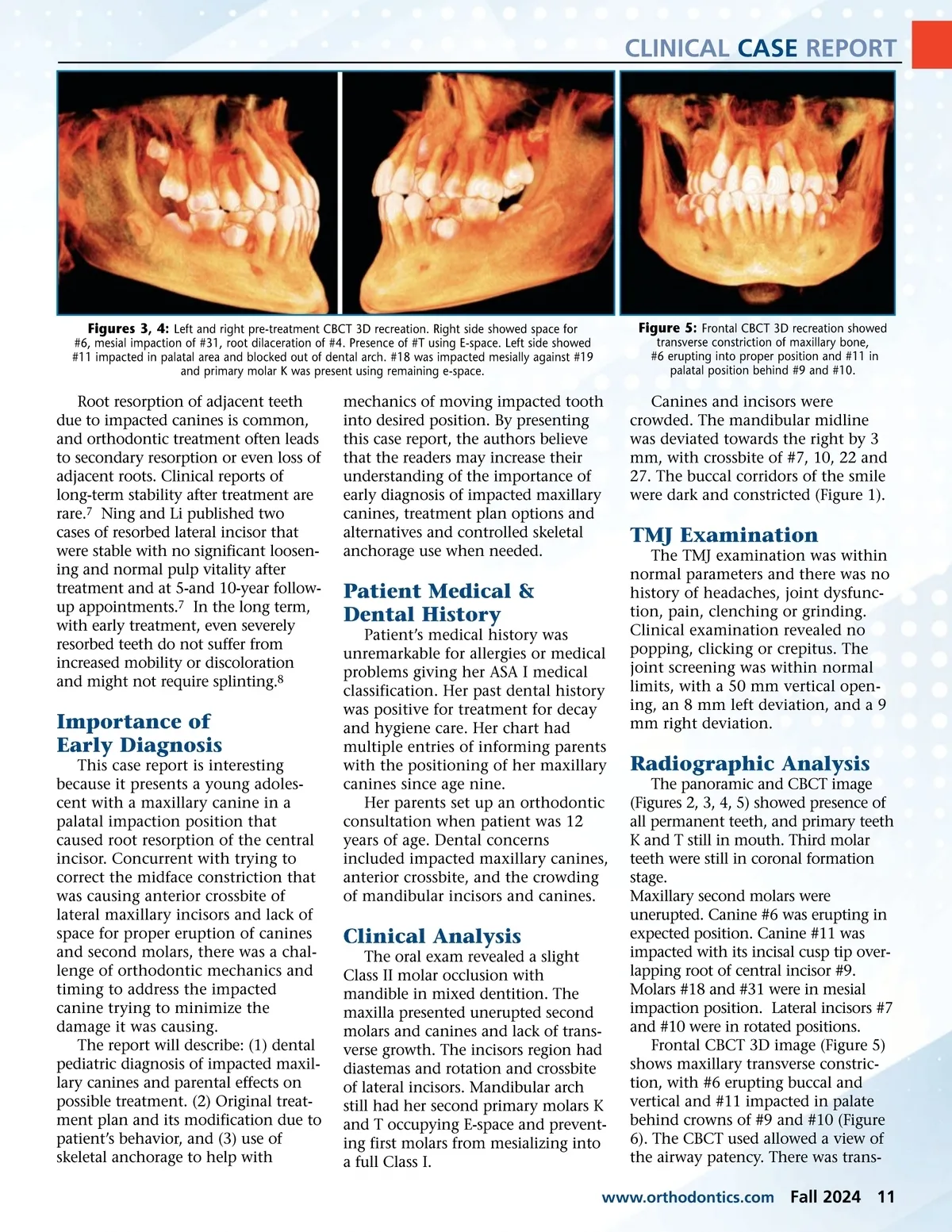
CLINICAL CASE REPORT Figures 3, 4: Left and right pre-treatment CBCT 3D recreation. Right side showed space for #6, mesial impaction of #31, root dilaceration of #4. Presence of #T using E-space. Left side showed #11 impacted in palatal area and blocked out of dental arch. #18 was impacted mesially against #19 and primary molar K was present using remaining e-space. Figure 5: Frontal CBCT 3D recreation showed transverse constriction of maxillary bone, #6 erupting into proper position and #11 in palatal position behind #9 and #10. Root resorption of adjacent teeth due to impacted canines is common, and orthodontic treatment often leads to secondary resorption or even loss of adjacent roots. Clinical reports of long-term stability after treatment are rare. 7 Ning and Li published two cases of resorbed lateral incisor that were stable with no significant loosen-ing and normal pulp vitality after treatment and at 5-and 10-year follow-up appointments. 7 In the long term, with early treatment, even severely resorbed teeth do not suffer from increased mobility or discoloration and might not require splinting. 8 mechanics of moving impacted tooth into desired position. By presenting this case report, the authors believe that the readers may increase their understanding of the importance of early diagnosis of impacted maxillary canines, treatment plan options and alternatives and controlled skeletal anchorage use when needed. Canines and incisors were crowded. The mandibular midline was deviated towards the right by 3 mm, with crossbite of #7, 10, 22 and 27. The buccal corridors of the smile were dark and constricted (Figure 1). TMJ Examination The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunc-tion, pain, clenching or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a 50 mm vertical open-ing, an 8 mm left deviation, and a 9 mm right deviation. Patient Medical & Dental History Patient’s medical history was unremarkable for allergies or medical problems giving her ASA I medical classification. Her past dental history was positive for treatment for decay and hygiene care. Her chart had multiple entries of informing parents with the positioning of her maxillary canines since age nine. Her parents set up an orthodontic consultation when patient was 12 years of age. Dental concerns included impacted maxillary canines, anterior crossbite, and the crowding of mandibular incisors and canines. Importance of Early Diagnosis This case report is interesting because it presents a young adoles-cent with a maxillary canine in a palatal impaction position that caused root resorption of the central incisor. Concurrent with trying to correct the midface constriction that was causing anterior crossbite of lateral maxillary incisors and lack of space for proper eruption of canines and second molars, there was a chal-lenge of orthodontic mechanics and timing to address the impacted canine trying to minimize the damage it was causing. The report will describe: (1) dental pediatric diagnosis of impacted maxil-lary canines and parental effects on possible treatment. (2) Original treat-ment plan and its modification due to patient’s behavior, and (3) use of skeletal anchorage to help with Radiographic Analysis The panoramic and CBCT image (Figures 2, 3, 4, 5) showed presence of all permanent teeth, and primary teeth K and T still in mouth. Third molar teeth were still in coronal formation stage. Maxillary second molars were unerupted. Canine #6 was erupting in expected position. Canine #11 was impacted with its incisal cusp tip over-lapping root of central incisor #9. Molars #18 and #31 were in mesial impaction position. Lateral incisors #7 and #10 were in rotated positions. Frontal CBCT 3D image (Figure 5) shows maxillary transverse constric-tion, with #6 erupting buccal and vertical and #11 impacted in palate behind crowns of #9 and #10 (Figure 6). The CBCT used allowed a view of the airway patency. There was trans-Clinical Analysis The oral exam revealed a slight Class II molar occlusion with mandible in mixed dentition. The maxilla presented unerupted second molars and canines and lack of trans-verse growth. The incisors region had diastemas and rotation and crossbite of lateral incisors. Mandibular arch still had her second primary molars K and T occupying E-space and prevent-ing first molars from mesializing into a full Class I. www.orthodontics.com Fall 2024 11
Journal of the American Orthodontic Society Fall 2024: Page 11