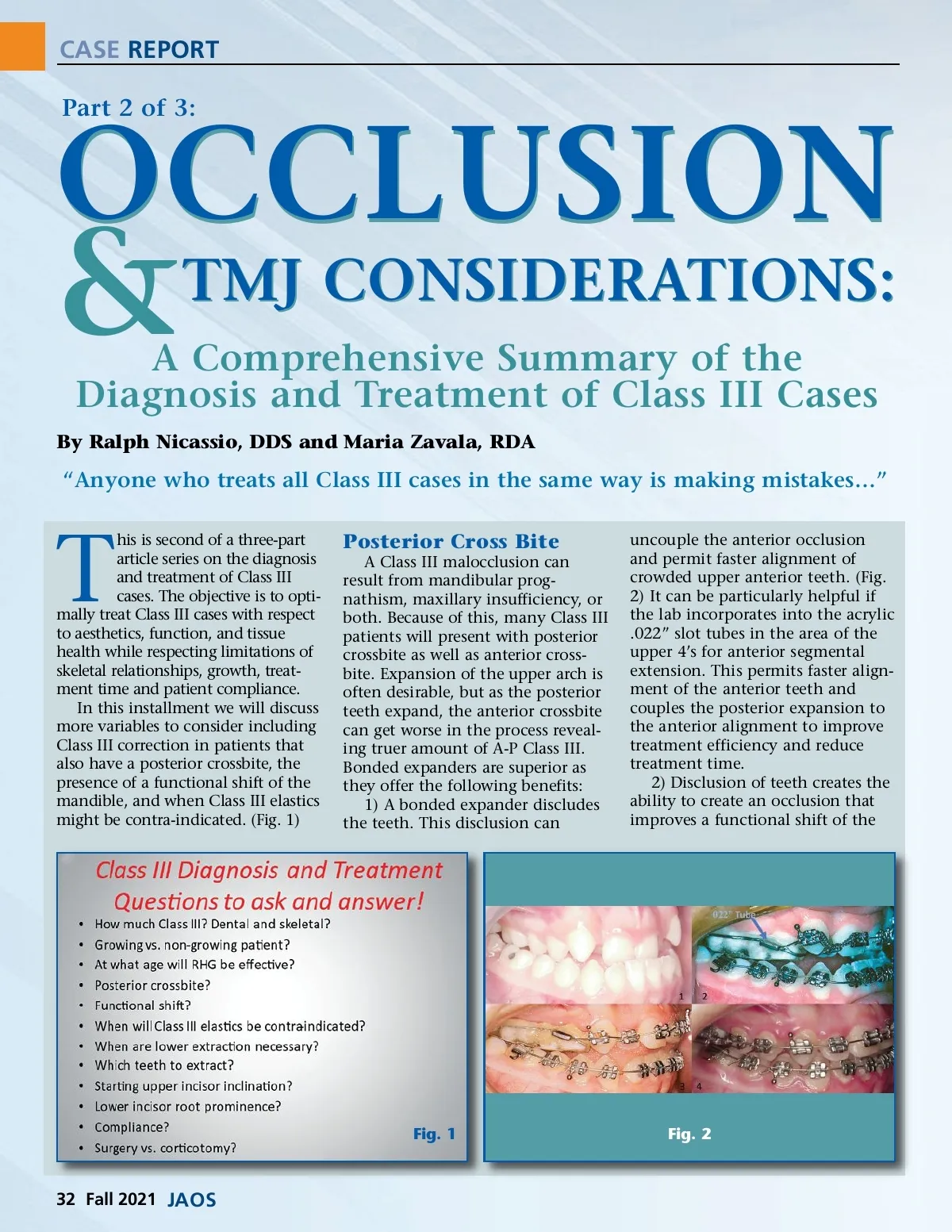
CASE REPORT OCCLUSION Part 2 of 3: & TMJ CONSIDERATIONS: A Comprehensive Summary of the Diagnosis and Treatment of Class III Cases By Ralph Nicassio, DDS and Maria Zavala, RDA “Anyone who treats all Class III cases in the same way is making mistakes…” T his is second of a three-part article series on the diagnosis and treatment of Class III cases. The objective is to opti-mally treat Class III cases with respect to aesthetics, function, and tissue health while respecting limitations of skeletal relationships, growth, treat-ment time and patient compliance. In this installment we will discuss more variables to consider including Class III correction in patients that also have a posterior crossbite, the presence of a functional shift of the mandible, and when Class III elastics might be contra-indicated. (Fig. 1) Posterior Cross Bite A Class III malocclusion can result from mandibular prog-nathism, maxillary insufficiency, or both. Because of this, many Class III patients will present with posterior crossbite as well as anterior cross-bite. Expansion of the upper arch is often desirable, but as the posterior teeth expand, the anterior crossbite can get worse in the process reveal-ing truer amount of A-P Class III. Bonded expanders are superior as they offer the following benefits: 1) A bonded expander discludes the teeth. This disclusion can uncouple the anterior occlusion and permit faster alignment of crowded upper anterior teeth. (Fig. 2) It can be particularly helpful if the lab incorporates into the acrylic .022” slot tubes in the area of the upper 4’s for anterior segmental extension. This permits faster align-ment of the anterior teeth and couples the posterior expansion to the anterior alignment to improve treatment efficiency and reduce treatment time. 2) Disclusion of teeth creates the ability to create an occlusion that improves a functional shift of the Fig. 1 Fig. 2 32 Fall 2021 JAOS
Journal of the American Orthodontic Society Fall 2021: Page 32