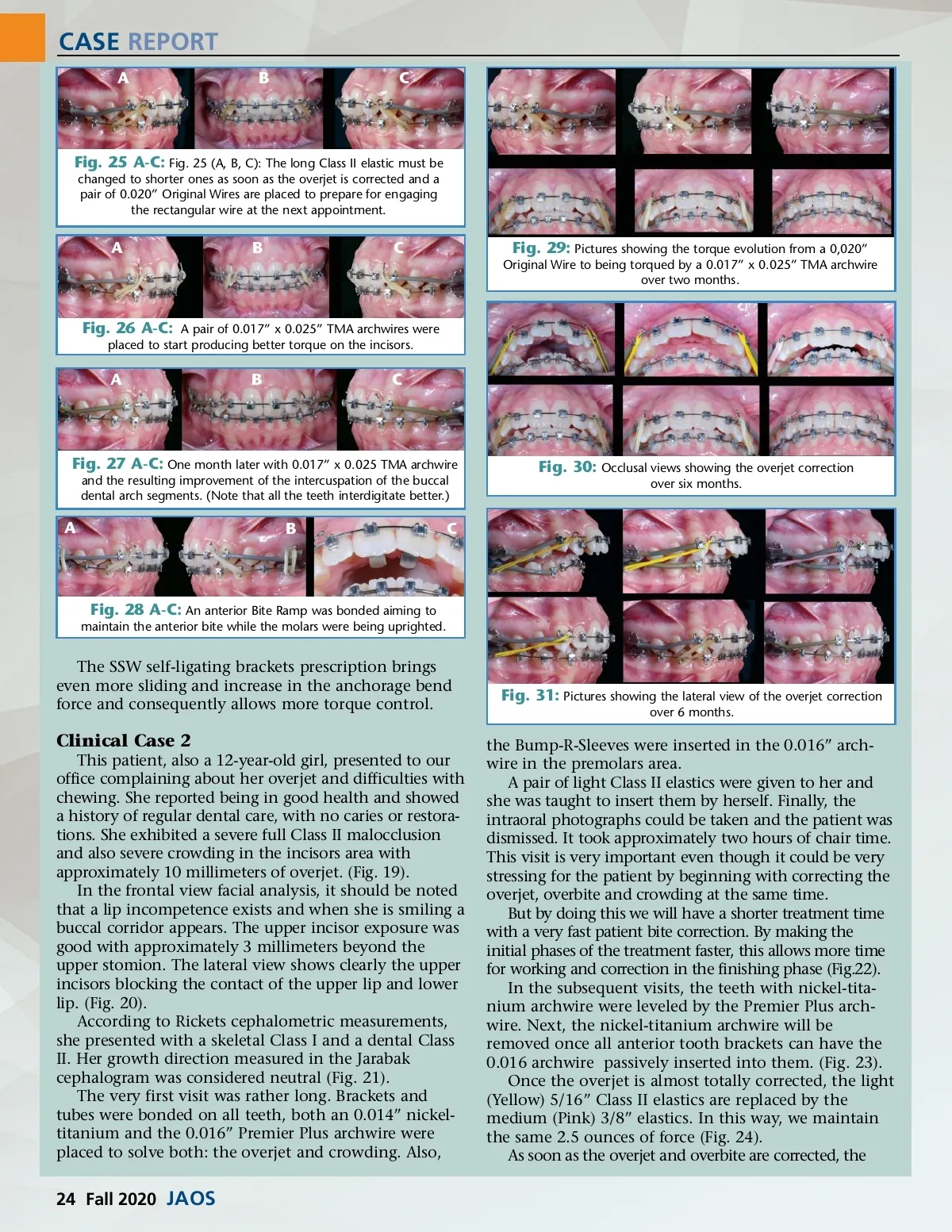
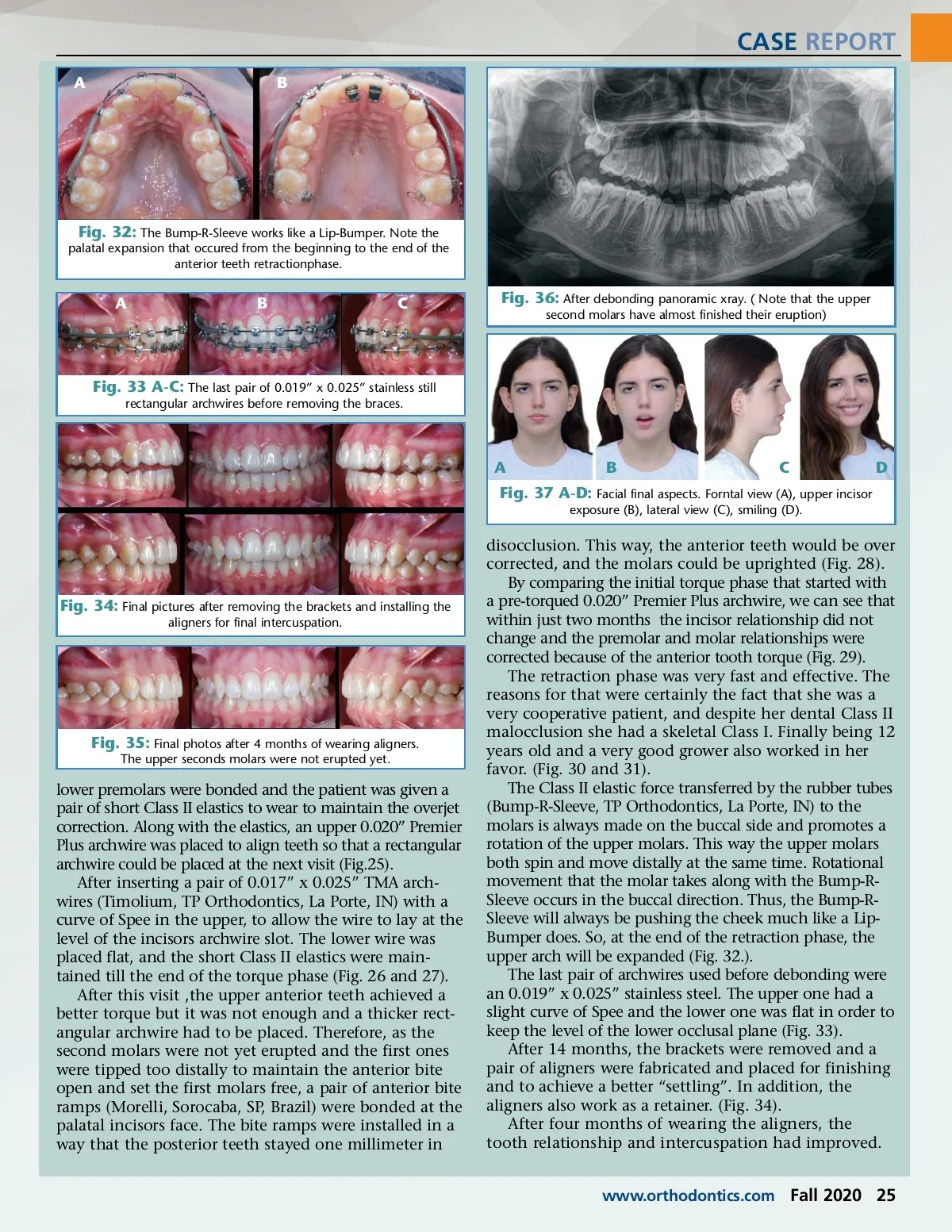
CASE REPORT ABC Fig. 25 A-C: Fig. 25 (A, B, C): The long Class II elastic must be changed to shorter ones as soon as the overjet is corrected and a pair of 0.020” Original Wires are placed to prepare for engaging the rectangular wire at the next appointment. ABC Fig. 29: Pictures showing the torque evolution from a 0,020” Original Wire to being torqued by a 0.017” x 0.025” TMA archwire over two months. Fig. 26 A-C: A pair of 0.017” x 0.025” TMA archwires were placed to start producing better torque on the incisors. ABC Fig. 27 A-C: One month later with 0.017” x 0.025 TMA archwire and the resulting improvement of the intercuspation of the buccal dental arch segments. (Note that all the teeth interdigitate better.) Fig. 30: Occlusal views showing the overjet correction over six months. A BC Fig. 28 A-C: An anterior Bite Ramp was bonded aiming to maintain the anterior bite while the molars were being uprighted. The SSW self-ligating brackets prescription brings even more sliding and increase in the anchorage bend force and consequently allows more torque control. Fig. 31: Pictures showing the lateral view of the overjet correction over 6 months. Clinical Case 2 This patient, also a 12-year-old girl, presented to our office complaining about her overjet and difficulties with chewing. She reported being in good health and showed a history of regular dental care, with no caries or restora-tions. She exhibited a severe full Class II malocclusion and also severe crowding in the incisors area with approximately 10 millimeters of overjet. (Fig. 19). In the frontal view facial analysis, it should be noted that a lip incompetence exists and when she is smiling a buccal corridor appears. The upper incisor exposure was good with approximately 3 millimeters beyond the upper stomion. The lateral view shows clearly the upper incisors blocking the contact of the upper lip and lower lip. (Fig. 20). According to Rickets cephalometric measurements, she presented with a skeletal Class I and a dental Class II. Her growth direction measured in the Jarabak cephalogram was considered neutral (Fig. 21). The very first visit was rather long. Brackets and tubes were bonded on all teeth, both an 0.014” nickel-titanium and the 0.016” Premier Plus archwire were placed to solve both: the overjet and crowding. Also, the Bump-R-Sleeves were inserted in the 0.016” arch-wire in the premolars area. A pair of light Class II elastics were given to her and she was taught to insert them by herself. Finally, the intraoral photographs could be taken and the patient was dismissed. It took approximately two hours of chair time. This visit is very important even though it could be very stressing for the patient by beginning with correcting the overjet, overbite and crowding at the same time. But by doing this we will have a shorter treatment time with a very fast patient bite correction. By making the initial phases of the treatment faster, this allows more time for working and correction in the finishing phase (Fig.22). In the subsequent visits, the teeth with nickel-tita-nium archwire were leveled by the Premier Plus arch-wire. Next, the nickel-titanium archwire will be removed once all anterior tooth brackets can have the 0.016 archwire passively inserted into them. (Fig. 23). Once the overjet is almost totally corrected, the light (Yellow) 5/16” Class II elastics are replaced by the medium (Pink) 3/8” elastics. In this way, we maintain the same 2.5 ounces of force (Fig. 24). As soon as the overjet and overbite are corrected, the 24 Fall 2020 JAOS
Journal of the American Orthodontic Society Fall 2020: Page 24