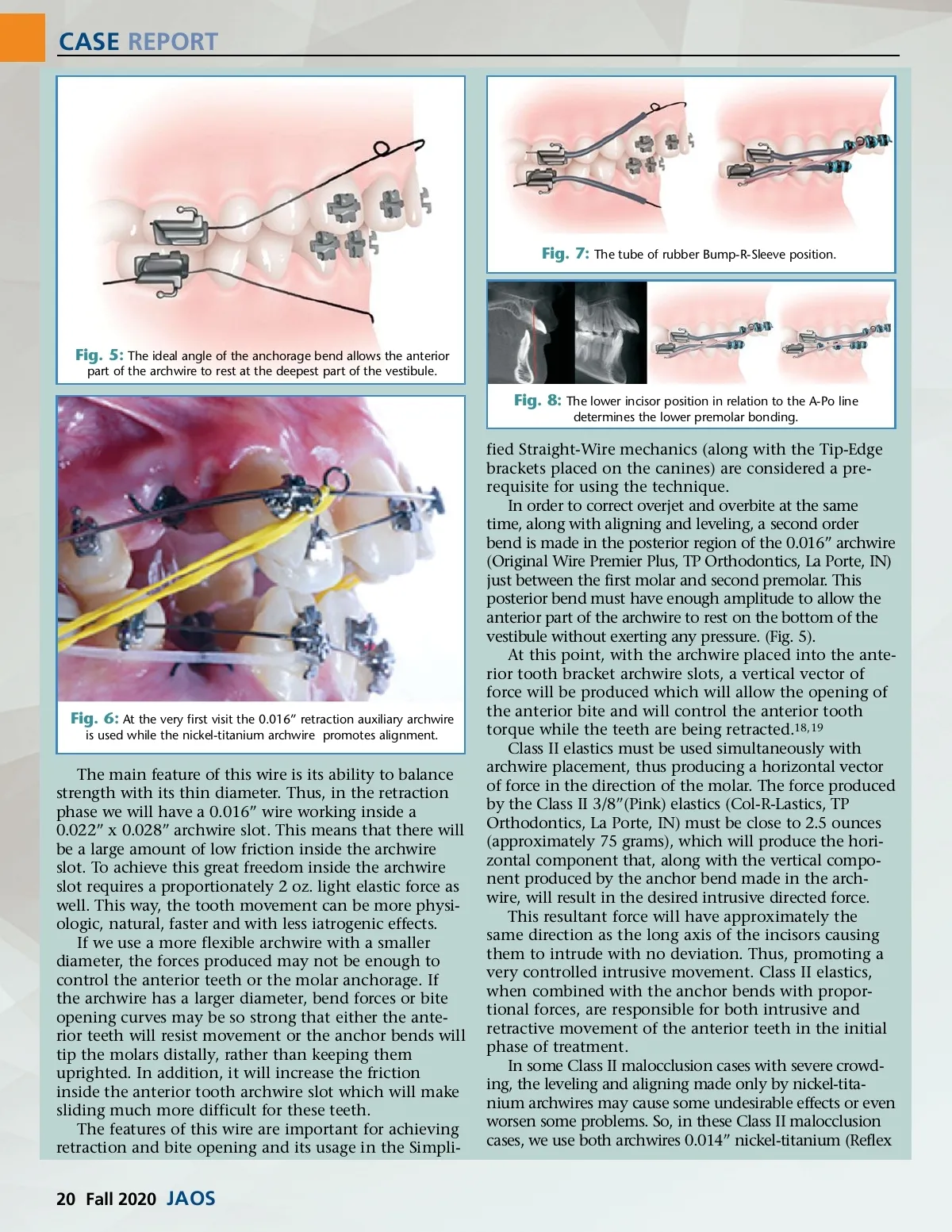
CASE REPORT Wire, TP Orthodontics, La Porte, IN) and 0.016” Original Wire Premier Plus archwires simultaneously. The 0.014” nickel-titanium must be placed in all the teeth and the 0.016” steel wire is placed in those teeth that it can fit in passively, with no deflection. Thus, in a short period, besides the leveling and alignment, the correction of the anteroposterior relationship and bite opening are also achieved simultaneously. This is possi-ble because of the posterior anchor bend that is made in the 0.016” Premier Plus along with the use of Class II elastics. And it does not matter if the treatment plan is for extraction or non-extraction treatment. (Fig. 6). An alternative treatment to be used to make sure that the teeth will move loosely and distally, involves making sure that the Premier Plus 0.016” archwire after being fixed must not be locked to the brackets. In order to make sure this is happening, we must pinch the pliers in the circles (these were made in the archwire for inserting the Class II elastics) near the canines and try to move the archwire towards the mesial or distal. If the archwire does not slide it is probably locked at some point. If this occurs, we must locate where the archwire is locked. We also insert in the posterior part of the 0.016” arch-wire a piece of sliding rubber tube that covers the archwire. It is placed between the canines and the molars. This rubber tube (Bump-R-Sleeve, TP Orthodontics, La Porte, IN) will transmit the force produced by Class II elastics at the region of the upper anterior teeth to the upper molars. Thus, Class II elastics may not only stimulate mandible growth, but also restrain the mesial movement of the upper molar, similar to what occurs with extraoral appliances. (Fig. 7) A BC Fig. 9: (A, B, C): Intra-oral views show a ¾ Class II malocclusion in both sizes. AB C D E Fig. 10: Frontal view (A), upper incisor exposure (B), smiling (C), lateral view with forced lip posture (D), lateral view unforced lip posture (E). The Lower Incisors Position In cases in which the lower incisors are tipping backwards (behind the A-Po line) the Bump-R-Sleeve tube can also be used between the anterior teeth and the molars in the lower arch in order to speed up both the protrusion of the lower incisors and the correction of the Class II relationship. Thus, beyond the stimulation of mandible growth it promotes some dental compensation. On the other hand, for those cases in which the incisors are at acceptable limits in relation to the A-Po line, the lower dental arch must be stabilized with rect-angular archwires to avoid the lower incisors protrud-ing movement. Under these conditions, the lower premolars should be bonded, and the Class II elastics retraction mechanics must not start until the 0.016” Premier Plus archwire can be placed passively on the premolars brackets. In subsequent visits, this archwire must be replaced by thicker ones until it is possible to place a rectangular 0.019” x 0.025” archwire. For cases in which lower incisors are beyond 3 mm ahead of the A-Po line, the correction of a Class II rela-tionship must be performed with other mechanics or appliances. Under these conditions, there are few options for treatment without extractions. Besides the mechanics of Class II elastics, functional orthopedic appliances in general, and the Herbst appliance in particular do produce the undesirable effect of protrud-ing the lower incisors. Certainly, the option for a treat-ment plan involving extraction is only decided upon once the patient profile is also analyzed (Fig. 8). At the end of overjet and overbite correction when the lingual faces of the upper incisors start touching the lower incisor’s buccal faces, the long Class II elastics must be replaced with shorter Class II 3/16” (Gray) elas-tics (Col-R-Lastics, TP Orthodontics, La Porte, IN) that deliver close to 1.5 ounces (approximately 50 grams). This short elastic is placed on the anterior upper arch-wire hook and on the first premolar lower bracket. Its function is to maintain the overjet and overbite correc-tion while the thicker upper archwires are promoting torque on the incisors. It disperses a very light force because it stretches just a small amount of area. In the SSW prescription of brackets, the incisor brack-ets are conventional straight-wire. As soon as the first rectangular archwire is inserted in their archwire slots, the torque correction immediately starts. We must avoid the undesirable effects that can happen when torque correc-tion begins, like diastemas, overjets and overbite relapse. To avoid those problems, a curve of Spee must be made in the upper rectangular archwire along with wearing of the short Class II elastics. This curve in the archwire combined with the short Class II elastics will maintain the overjet and overbite correction, achieved by the previ-ously phase while the ideal incisor torque is obtained. Clinical Case I The patient, a 12-year, 5-month-old girl came to our office complaining about her overjet and the injury that the upper incisors were causing to her lower lip. She reported being in good health and showed a history of regular dental care with no caries or restora-tions. She also exhibited a skeletal and dental Class II and she did not present with any other issues including jaw function, which showed normal range of motion. There was no pain on palpation of her jaw joints and no joint sounds with opening and closing. (Fig. 9). www.orthodontics.com Fall 2020 21
Journal of the American Orthodontic Society Fall 2020: Page 21