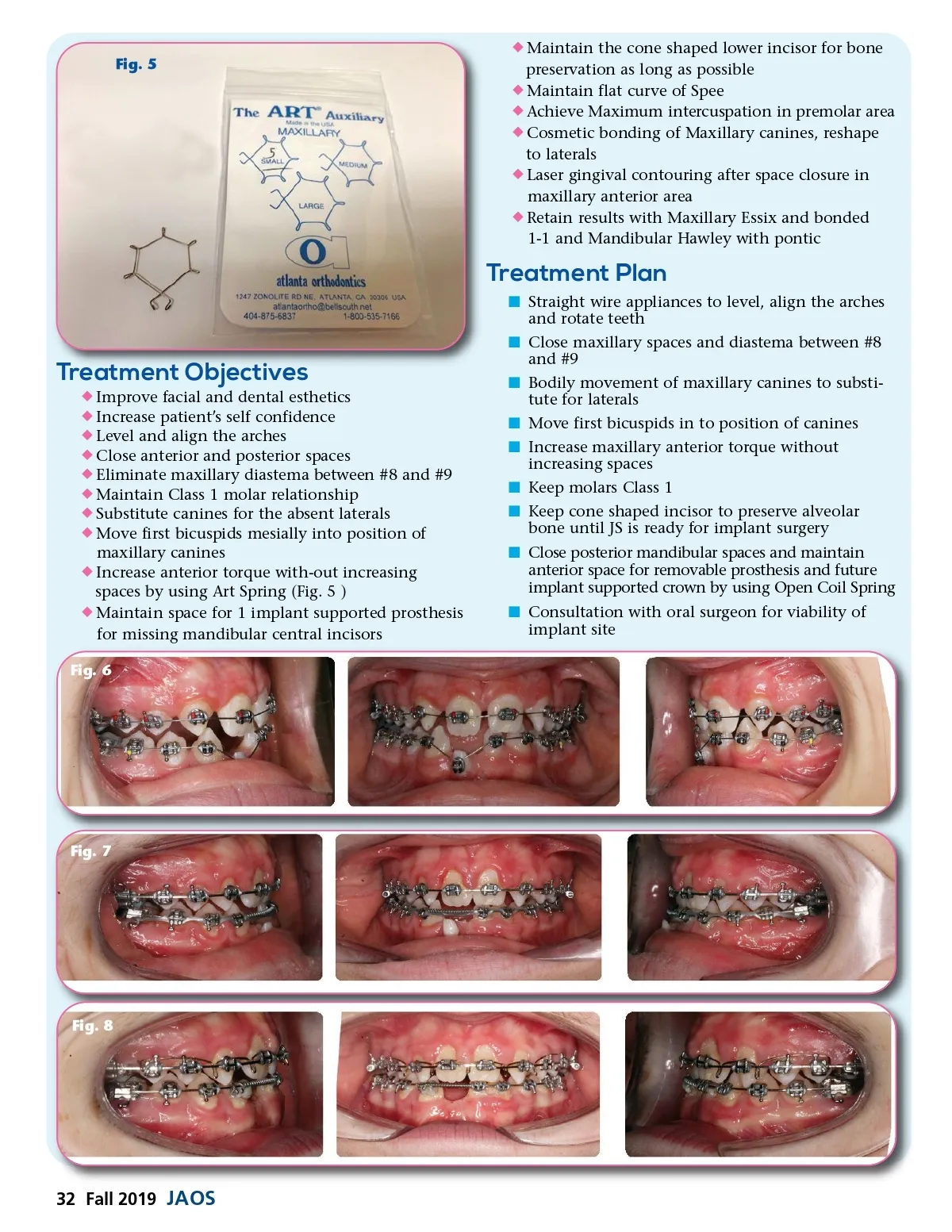
Fig. 10 Fig. 9 "At the de-banding appointment once the appliances were removed, the maxillary canines were shaped and bonded by direct composite technique to resemble maxillary laterals. JS also had maxillary gingival hyperplasia due to poor oral hygiene and using power chain to close spaces. This condition was treated with Nd:Yag and Er:yag laser gingival contouring. The use of lasers allowed for a bloodless gingivectomy procedure to improve esthetics and retainer fit." months of leveling, it was noticed that the cone shaped tooth was not moving due to ankylosis and compro-mised the alignment of other teeth. Thus, it was bypassed and left in the arch for alveolar bone preserva-tion. However, JS did not like the protruded appearance of that tooth specially that it was hurting his lip. The malformed incisor had to be extracted and the space maintained with an open coil spring. (Fig.7) As JS progressed in to 0.016-0.020 stainless steel wire series, power chain was used to close the spaces between maxillary incisors and bodily mesialize maxil-lary canines. He progressed to 0.019 x 0.025 thermal and 0.021 x 0.25ss using an Art auxillary spring (Atlanta Orhtodontics) to increase the torque of incisors and used power chain to consolidate spaces. (Fig. 8). Due to strong Class III skeletal growth, the lower arch was maintained in 0.020 ss round wires and the canines were retracted using Class III elastics. Mandibular spaces were closed by using power chain and cinch back in the lower wires and open coil spring to maintain implant space. Three weeks prior to debonding, a mandibular algi-nate impression was taken for fabrication of a Hawley retainer with pontics for teeth #24 and #25 to be deliv-ered at the time of debonding. At the de-banding appointment once the appliances were removed, the maxillary canines were shaped and bonded by direct composite technique to resemble maxillary laterals. JS also had maxillary gingival hyperplasia due to poor oral hygiene and using power chain to close spaces. This condition was treated with Nd:Yag and Er:yag laser gingival contouring. The use of lasers allowed for a bloodless gingivectomy procedure to improve esthetics and retainer fit. (Fig.9 Final post-Tx Montage). Once the esthetic and surgical finishing touches were placed, teeth #8 and #9 were bonded with affixed lingual wire and the upper arch was impressed for a maxillary Essix retainer. (Fig. 10) The length of active treatment time was about 25 months. www.orthodontics.com í Monitor eruption of maxillary second molars í Laser gingivectomy to contour hyperplastic maxil-lary gingiva í Hawley with pontic for mandibular retention í See the patient periodically to monitor growth í Estimated treatment time: 24 months Case Summary and Analysis Initially, the patient was offered two treatment plans for the maxillary arch. Our first option was to distalize the maxillary canines and open up spaces for two implants to replace the congenitally missing laterals once the patient reached dentofacial matu-rity. With this option, he would have either two Maryland Bridges or a removable partial denture with Pontics as an interim prosthesis during his growing years. The second option was canine substitution in the maxillary arch by closing the spaces and moving maxil-lary canines to replace the laterals. Later on, JS would receive cosmetic bonding and reshaping of the canines for maximum esthetic results. This option would eliminate the need for implants or removable dentures in the future. The treatment for the lower arch consisted of maintaining a single implant space for a future fixed prosthesis with an interim removable Hawley retainer with Pontic. After reviewing the pros and cons of these treatment plans, the patient and mother decided on the non-implant option and canine substitution to minimize the number of pros-thesis and surgical intervention in the maxillary arch. Treatment started by banding the first molars and bracketing all the teeth including the cone shaped incisor (Fig.6 Initial banding 9/12/16). Once we started leveling and aligning the teeth using 0.014-.018 Niti wire series, JS started to have pain. Discomfort was mainly related to the sharp cone-shaped tooth on the lower anterior area. After a few Fall 2019 33
Journal of the American Orthodontic Society Fall 2019: Page 33