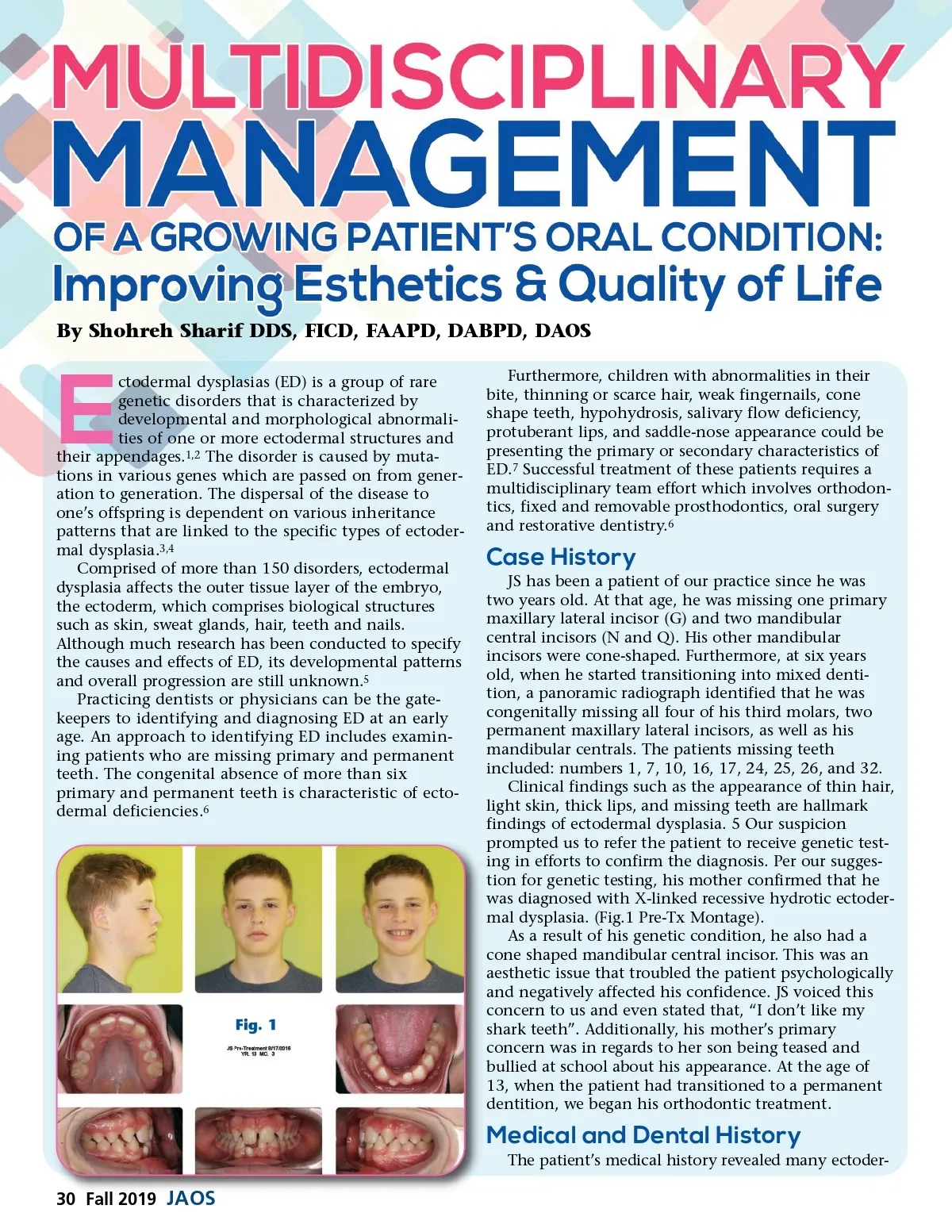
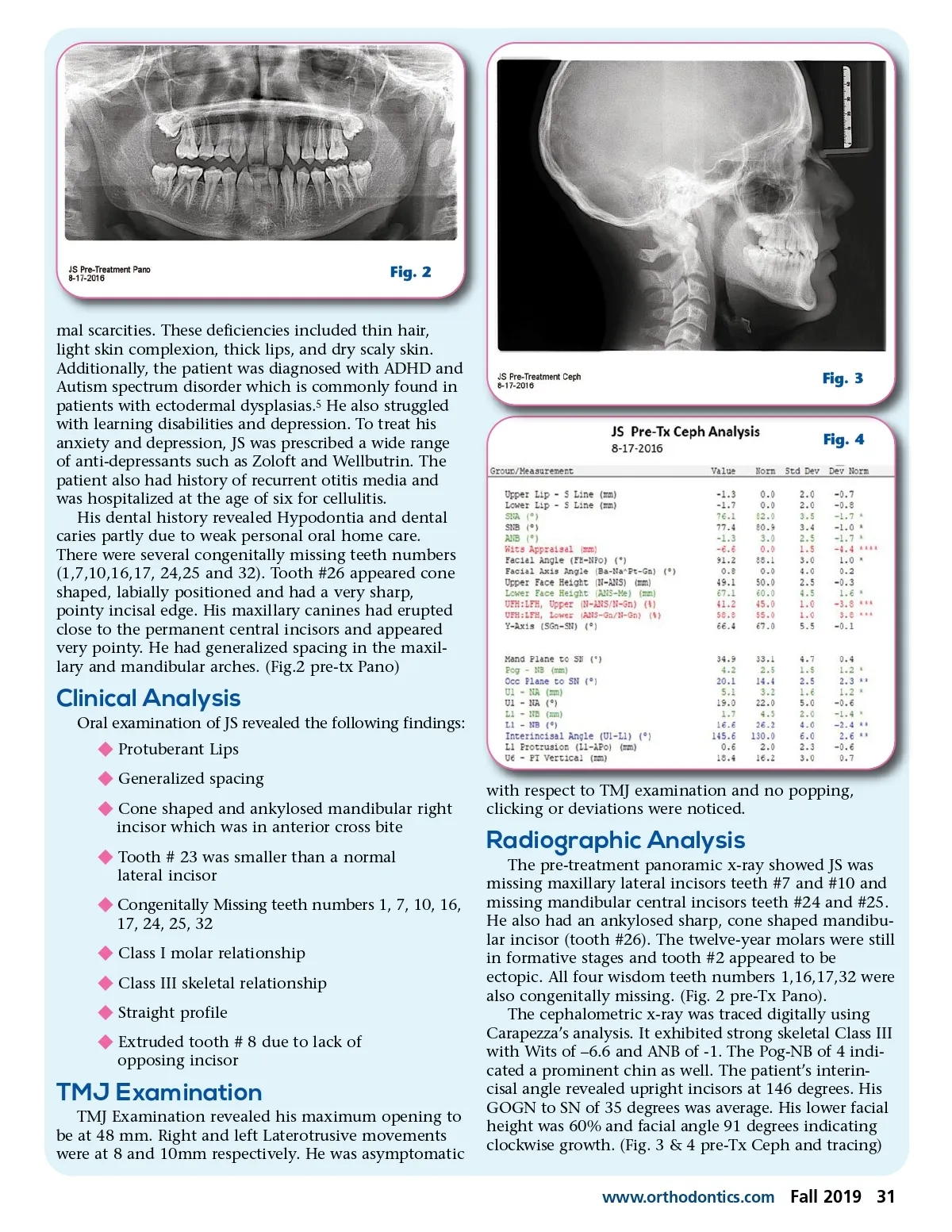
Fig. 2 mal scarcities. These deficiencies included thin hair, light skin complexion, thick lips, and dry scaly skin. Additionally, the patient was diagnosed with ADHD and Autism spectrum disorder which is commonly found in patients with ectodermal dysplasias. 5 He also struggled with learning disabilities and depression. To treat his anxiety and depression, JS was prescribed a wide range of anti-depressants such as Zoloft and Wellbutrin. The patient also had history of recurrent otitis media and was hospitalized at the age of six for cellulitis. His dental history revealed Hypodontia and dental caries partly due to weak personal oral home care. There were several congenitally missing teeth numbers (1,7,10,16,17, 24,25 and 32). Tooth #26 appeared cone shaped, labially positioned and had a very sharp, pointy incisal edge. His maxillary canines had erupted close to the permanent central incisors and appeared very pointy. He had generalized spacing in the maxil-lary and mandibular arches. (Fig.2 pre-tx Pano) Fig. 3 Fig. 4 Clinical Analysis Oral examination of JS revealed the following findings: v Protuberant Lips v Generalized spacing v Cone shaped and ankylosed mandibular right incisor which was in anterior cross bite v Tooth # 23 was smaller than a normal lateral incisor v Congenitally Missing teeth numbers 1, 7, 10, 16, 17, 24, 25, 32 v Class I molar relationship v Class III skeletal relationship v Straight profile v Extruded tooth # 8 due to lack of opposing incisor with respect to TMJ examination and no popping, clicking or deviations were noticed. Radiographic Analysis The pre-treatment panoramic x-ray showed JS was missing maxillary lateral incisors teeth #7 and #10 and missing mandibular central incisors teeth #24 and #25. He also had an ankylosed sharp, cone shaped mandibu-lar incisor (tooth #26). The twelve-year molars were still in formative stages and tooth #2 appeared to be ectopic. All four wisdom teeth numbers 1,16,17,32 were also congenitally missing. (Fig. 2 pre-Tx Pano). The cephalometric x-ray was traced digitally using Carapezza’s analysis. It exhibited strong skeletal Class III with Wits of –6.6 and ANB of -1. The Pog-NB of 4 indi-cated a prominent chin as well. The patient’s interin-cisal angle revealed upright incisors at 146 degrees. His GOGN to SN of 35 degrees was average. His lower facial height was 60% and facial angle 91 degrees indicating clockwise growth. (Fig. 3 & 4 pre-Tx Ceph and tracing) www.orthodontics.com TMJ Examination TMJ Examination revealed his maximum opening to be at 48 mm. Right and left Laterotrusive movements were at 8 and 10mm respectively. He was asymptomatic Fall 2019 31
Journal of the American Orthodontic Society Fall 2019: Page 31