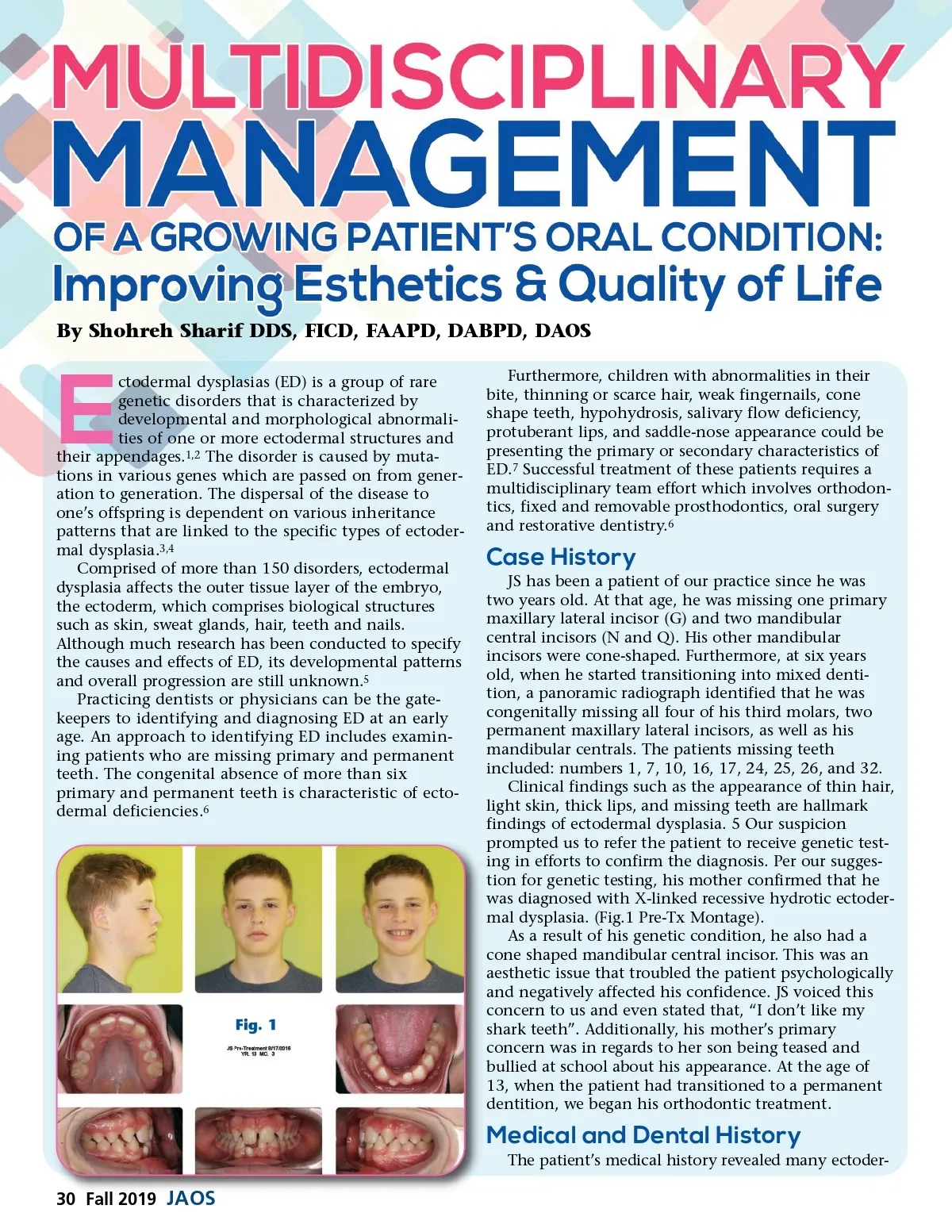
By Shohreh Sharif DDS, FICD, FAAPD, DABPD, DAOS ctodermal dysplasias (ED) is a group of rare genetic disorders that is characterized by developmental and morphological abnormali-ties of one or more ectodermal structures and their appendages. 1,2 The disorder is caused by muta-tions in various genes which are passed on from gener-ation to generation. The dispersal of the disease to one’s offspring is dependent on various inheritance patterns that are linked to the specific types of ectoder-mal dysplasia. 3,4 Comprised of more than 150 disorders, ectodermal dysplasia affects the outer tissue layer of the embryo, the ectoderm, which comprises biological structures such as skin, sweat glands, hair, teeth and nails. Although much research has been conducted to specify the causes and effects of ED, its developmental patterns and overall progression are still unknown. 5 Practicing dentists or physicians can be the gate-keepers to identifying and diagnosing ED at an early age. An approach to identifying ED includes examin-ing patients who are missing primary and permanent teeth. The congenital absence of more than six primary and permanent teeth is characteristic of ecto-dermal deficiencies. 6 E Furthermore, children with abnormalities in their bite, thinning or scarce hair, weak fingernails, cone shape teeth, hypohydrosis, salivary flow deficiency, protuberant lips, and saddle-nose appearance could be presenting the primary or secondary characteristics of ED. 7 Successful treatment of these patients requires a multidisciplinary team effort which involves orthodon-tics, fixed and removable prosthodontics, oral surgery and restorative dentistry. 6 Case History JS has been a patient of our practice since he was two years old. At that age, he was missing one primary maxillary lateral incisor (G) and two mandibular central incisors (N and Q). His other mandibular incisors were cone-shaped. Furthermore, at six years old, when he started transitioning into mixed denti-tion, a panoramic radiograph identified that he was congenitally missing all four of his third molars, two permanent maxillary lateral incisors, as well as his mandibular centrals. The patients missing teeth included: numbers 1, 7, 10, 16, 17, 24, 25, 26, and 32. Clinical findings such as the appearance of thin hair, light skin, thick lips, and missing teeth are hallmark findings of ectodermal dysplasia. 5 Our suspicion prompted us to refer the patient to receive genetic test-ing in efforts to confirm the diagnosis. Per our sugges-tion for genetic testing, his mother confirmed that he was diagnosed with X-linked recessive hydrotic ectoder-mal dysplasia. (Fig.1 Pre-Tx Montage). As a result of his genetic condition, he also had a cone shaped mandibular central incisor. This was an aesthetic issue that troubled the patient psychologically and negatively affected his confidence. JS voiced this concern to us and even stated that, “I don’t like my shark teeth”. Additionally, his mother’s primary concern was in regards to her son being teased and bullied at school about his appearance. At the age of 13, when the patient had transitioned to a permanent dentition, we began his orthodontic treatment. Fig. 1 Medical and Dental History The patient’s medical history revealed many ectoder-30 Fall 2019 JAOS
Journal of the American Orthodontic Society Fall 2019: Page 30