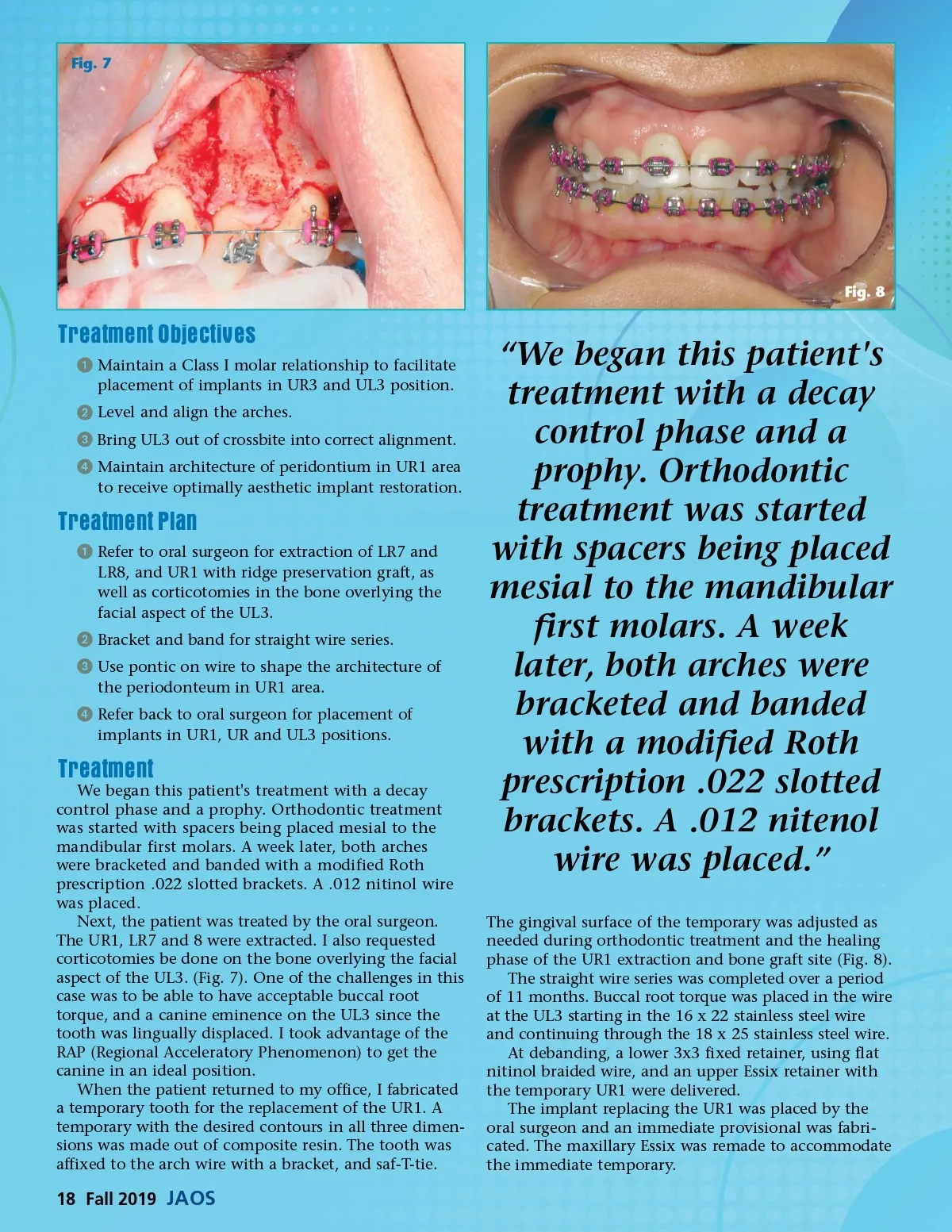
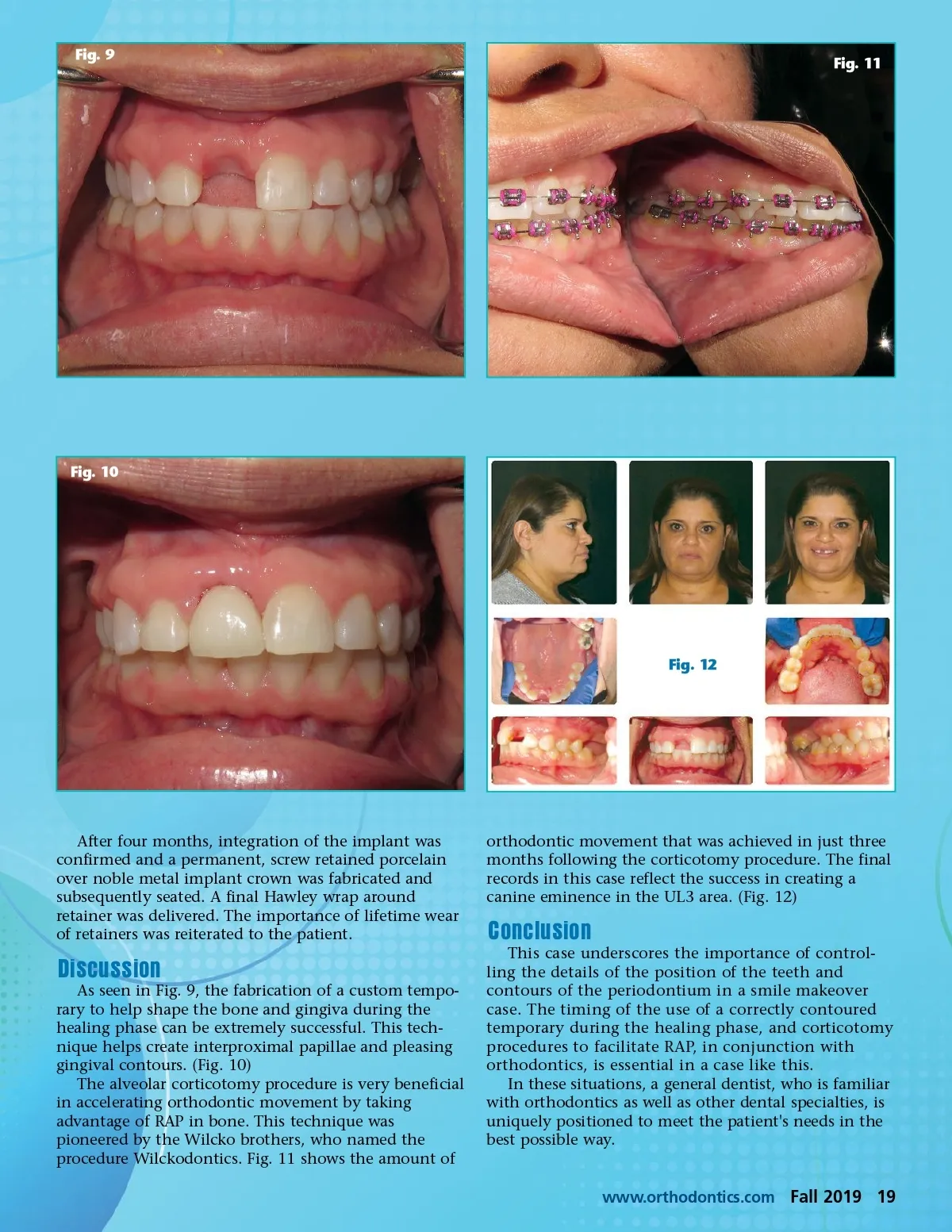
Fig. 7 Fig. 8 Treatment Objectives ᕡ Maintain a Class I molar relationship to facilitate placement of implants in UR3 and UL3 position. ᕢ Level and align the arches. ᕣ Bring UL3 out of crossbite into correct alignment. ᕤ Maintain architecture of peridontium in UR1 area to receive optimally aesthetic implant restoration. Treatment Plan ᕡ Refer to oral surgeon for extraction of LR7 and LR8, and UR1 with ridge preservation graft, as well as corticotomies in the bone overlying the facial aspect of the UL3. ᕢ Bracket and band for straight wire series. ᕣ Use pontic on wire to shape the architecture of the periodonteum in UR1 area. ᕤ Refer back to oral surgeon for placement of implants in UR1, UR and UL3 positions. Treatment We began this patient's treatment with a decay control phase and a prophy. Orthodontic treatment was started with spacers being placed mesial to the mandibular first molars. A week later, both arches were bracketed and banded with a modified Roth prescription .022 slotted brackets. A .012 nitinol wire was placed. Next, the patient was treated by the oral surgeon. The UR1, LR7 and 8 were extracted. I also requested corticotomies be done on the bone overlying the facial aspect of the UL3. (Fig. 7). One of the challenges in this case was to be able to have acceptable buccal root torque, and a canine eminence on the UL3 since the tooth was lingually displaced. I took advantage of the RAP (Regional Acceleratory Phenomenon) to get the canine in an ideal position. When the patient returned to my office, I fabricated a temporary tooth for the replacement of the UR1. A temporary with the desired contours in all three dimen-sions was made out of composite resin. The tooth was affixed to the arch wire with a bracket, and saf-T-tie. “We began this patient's treatment with a decay control phase and a prophy. Orthodontic treatment was started with spacers being placed mesial to the mandibular first molars. A week later, both arches were bracketed and banded with a modified Roth prescription .022 slotted brackets. A .012 nitenol wire was placed.” The gingival surface of the temporary was adjusted as needed during orthodontic treatment and the healing phase of the UR1 extraction and bone graft site (Fig. 8). The straight wire series was completed over a period of 11 months. Buccal root torque was placed in the wire at the UL3 starting in the 16 x 22 stainless steel wire and continuing through the 18 x 25 stainless steel wire. At debanding, a lower 3x3 fixed retainer, using flat nitinol braided wire, and an upper Essix retainer with the temporary UR1 were delivered. The implant replacing the UR1 was placed by the oral surgeon and an immediate provisional was fabri-cated. The maxillary Essix was remade to accommodate the immediate temporary. 18 Fall 2019 JAOS
Journal of the American Orthodontic Society Fall 2019: Page 18