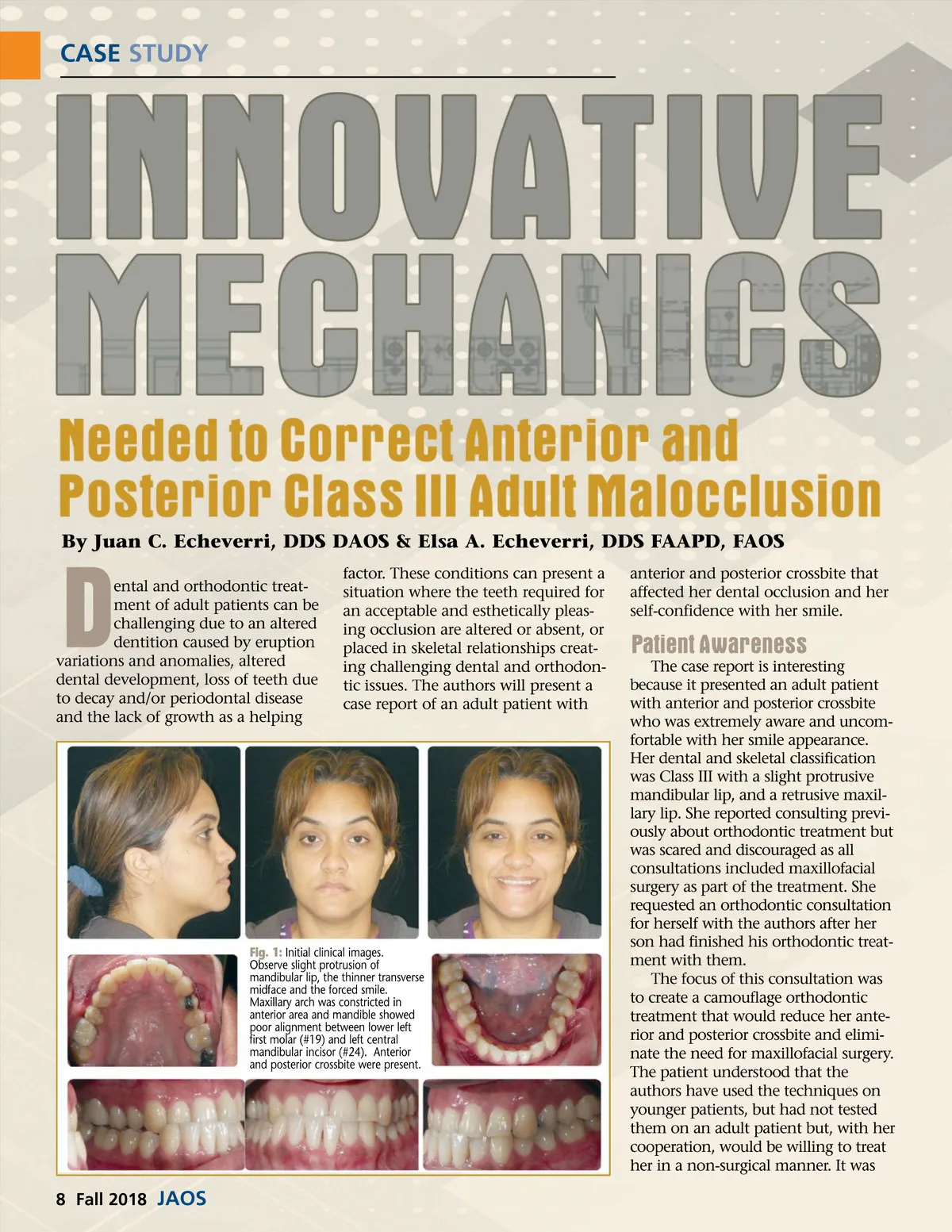
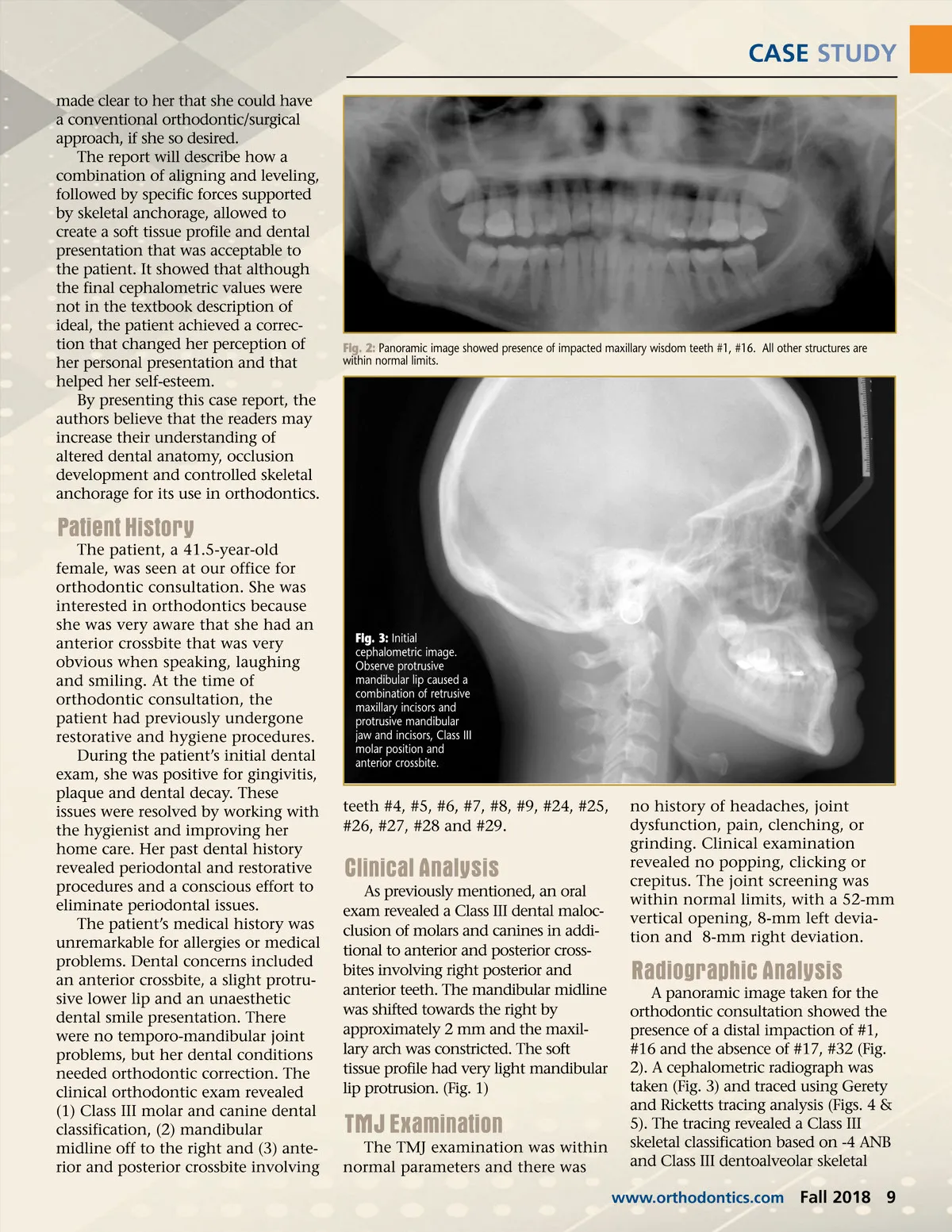
CASE STUDY made clear to her that she could have a conventional orthodontic/surgical approach, if she so desired. The report will describe how a combination of aligning and leveling, followed by specific forces supported by skeletal anchorage, allowed to create a soft tissue profile and dental presentation that was acceptable to the patient. It showed that although the final cephalometric values were not in the textbook description of ideal, the patient achieved a correc-tion that changed her perception of her personal presentation and that helped her self-esteem. By presenting this case report, the authors believe that the readers may increase their understanding of altered dental anatomy, occlusion development and controlled skeletal anchorage for its use in orthodontics. Fig. 2: Panoramic image showed presence of impacted maxillary wisdom teeth #1, #16. All other structures are within normal limits. Patient History The patient, a 41.5-year-old female, was seen at our office for orthodontic consultation. She was interested in orthodontics because she was very aware that she had an anterior crossbite that was very obvious when speaking, laughing and smiling. At the time of orthodontic consultation, the patient had previously undergone restorative and hygiene procedures. During the patient’s initial dental exam, she was positive for gingivitis, plaque and dental decay. These issues were resolved by working with the hygienist and improving her home care. Her past dental history revealed periodontal and restorative procedures and a conscious effort to eliminate periodontal issues. The patient’s medical history was unremarkable for allergies or medical problems. Dental concerns included an anterior crossbite, a slight protru-sive lower lip and an unaesthetic dental smile presentation. There were no temporo-mandibular joint problems, but her dental conditions needed orthodontic correction. The clinical orthodontic exam revealed (1) Class III molar and canine dental classification, (2) mandibular midline off to the right and (3) ante-rior and posterior crossbite involving Fig. 3: Initial cephalometric image. Observe protrusive mandibular lip caused a combination of retrusive maxillary incisors and protrusive mandibular jaw and incisors, Class III molar position and anterior crossbite. teeth #4, #5, #6, #7, #8, #9, #24, #25, #26, #27, #28 and #29. Clinical Analysis As previously mentioned, an oral exam revealed a Class III dental maloc-clusion of molars and canines in addi-tional to anterior and posterior cross-bites involving right posterior and anterior teeth. The mandibular midline was shifted towards the right by approximately 2 mm and the maxil-lary arch was constricted. The soft tissue profile had very light mandibular lip protrusion. (Fig. 1) no history of headaches, joint dysfunction, pain, clenching, or grinding. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a 52-mm vertical opening, 8-mm left devia-tion and 8-mm right deviation. Radiographic Analysis A panoramic image taken for the orthodontic consultation showed the presence of a distal impaction of #1, #16 and the absence of #17, #32 (Fig. 2). A cephalometric radiograph was taken (Fig. 3) and traced using Gerety and Ricketts tracing analysis (Figs. 4 & 5). The tracing revealed a Class III skeletal classification based on -4 ANB and Class III dentoalveolar skeletal www.orthodontics.com TMJ Examination The TMJ examination was within normal parameters and there was Fall 2018 9
Journal of the American Orthodontic Society Fall 2018: Page 9