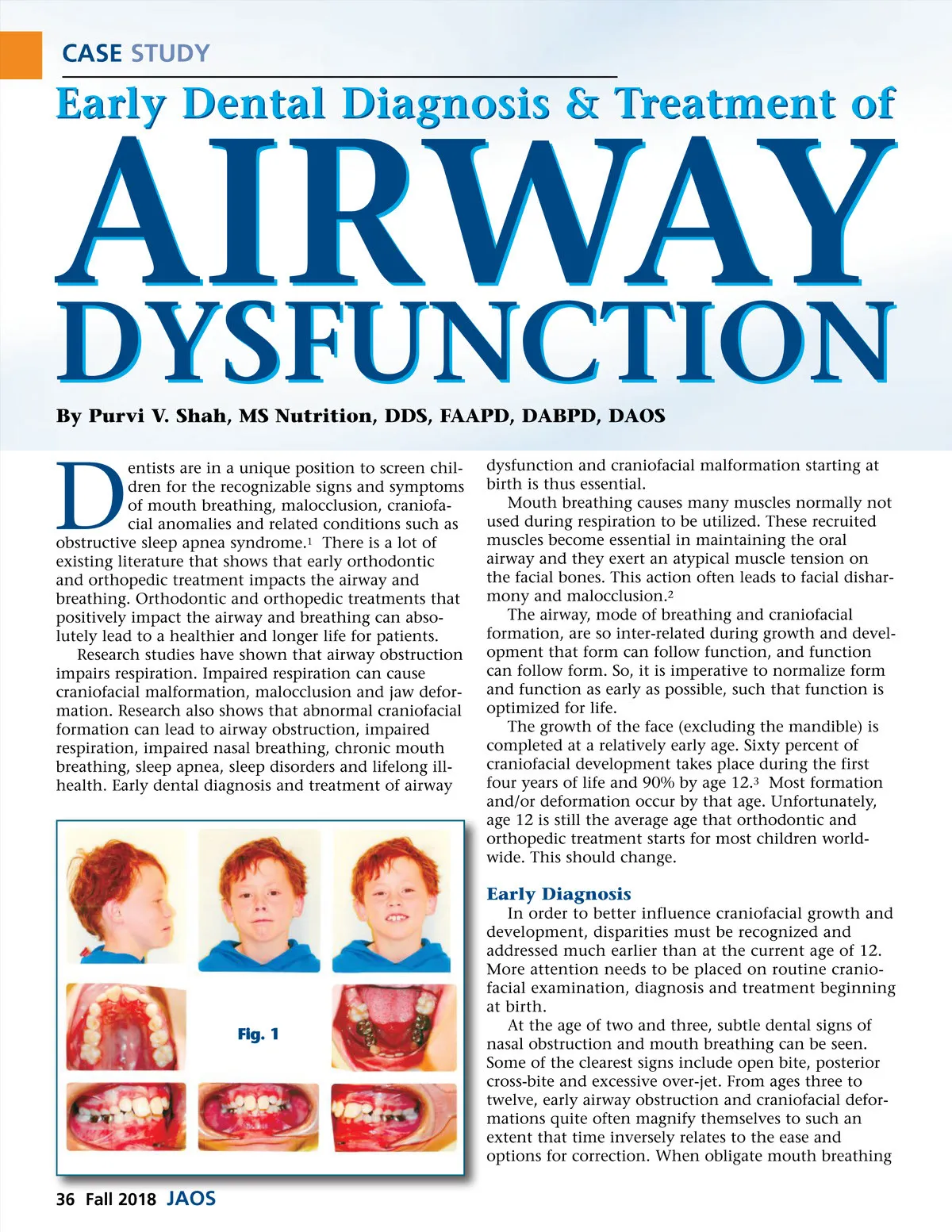
CASE STUDY is suspected, cephalometric analysis should be used to evaluate facial architecture to better recognize oral breathing caused dento-skeletal dysmorphia. Fig. 2 Early Treatment Early treatment is essential to normalizing growth and development. Early treatment maximizes the success of corrective orthodontics and orthopedics. Dental orthodontic appliances have been shown to improve the sagittal dimensions of the upper airway in children. 4 Dental rapid maxillary expansion has been shown to be a simple, conservative method of treating impaired nasal respiration in patients 4 years to 30 years, but the younger the patient the better the long term results. Dental maxillary expansion is an effective method for increasing the width of narrow maxillary arches and it also reduces nasal resistance from levels seen with mouth breath-ing to levels consistent with normal nasal respiration. 5 K.E.’s dental examination also established the following: ᕡ Mouth breathing ᕢ High appearing Narrow Palate Vault ᕣ Deep-Bite -Locked Occlusion / Mandible ᕤ Anterior Overjet ᕥ Posterior Cross-Bite ᕦ Class II Malocclusion ᕧ Short turned up maxillary lip ᕨ Dry mouth contributing to high caries risk factor Case Example K.E.’s Treatment at Age 8 Here is a case that provides evidence and support for early diagnosis and early treatment of malocclusion, craniofacial anomalies and related conditions such as Obstructive Sleep Apnea (OSA) syndrome. Correct orthodontic treatment, performed at the right time, cannot only create beautiful smiles but it can also help prevent and or cure children who are suffering from Sleep Disordered Breathing (SDB) or OSA. K.E. was a five-year-old red-haired Caucasian male with multiple cavities on his primary molars. He had been diagnosed with Attention Deficient Disorder (ADD) and asthma and exhibited high anxiety in the dental office. Per his mother, K.E. was doing better at our office than he ever had at any other dental office. This was evidenced by the fact that his mother was happy to drive for an hour and half from her home to bring K.E. to our office for his routine care. As K.E. got older and reached eight years of age, we noticed that his incisors were proclined. His mother also noticed the same and expressed concern about his flared “buck teeth” which was causing many children to tease and bully him at school. On evaluating his orthodontic records in combination with his medical history, it seemed quite clear that early orthodontic treatment could benefit K.E. Clinical Analysis ᕡ Posterior cross bite and a locked occlusion due to a deep bite. ᕢ A ½ Class II molar relationship, a 90% overbite, and 5mm overjet. ᕣ A classic mixed dentition with multiple restorations. ᕤ A mouth breather, and lip incompetence. ᕥ Mesocephalic and a straight profile. Fig. 1 (Pre Txt Montage) TMJ Examination ᕡ TMJ examination revealed that his vertical open-ing was 45 mm. ᕢ Right and left laterotrusive movements measured 7 mm’s on both sides. ᕣ K.E. stated that he was not experiencing any pain ᕤ There was no popping or clicking or deviations. Medical and Dental History K.E.’s medical history included the following: ᕡ Swollen tonsils and adenoids ᕢ Frequent ear and upper respiratory infections ᕣ Severe allergies and Asthma ᕤ Disrupted sleep pattern ᕥ ADD / ADHD related behavioral issues Radiographic Analysis The panoramic x-ray showed a full complement mixed dentition teeth. There were composite white fill-ings on the upper primary molars and stainless steel crowns on the lower primary molars. As K.E. was eight years old, the third molars were not yet formed. His bone density appeared to be normal. (Fig. 2) www.orthodontics.com Fall 2018 37
Journal of the American Orthodontic Society Fall 2018: Page 37