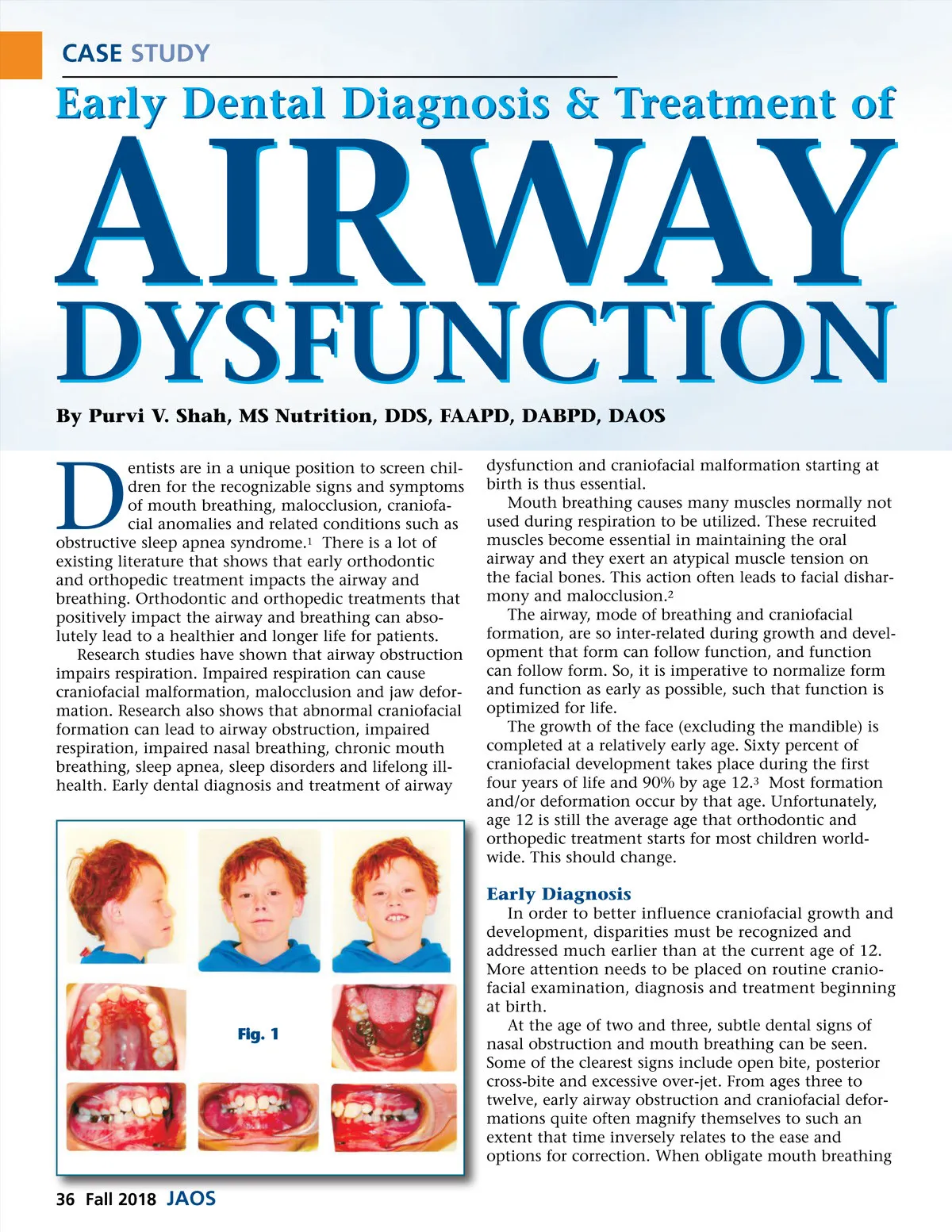
CASE STUDY Early Dental Diagnosis & Treatment of AIRWAY DYSFUNCTION By Purvi V. Shah, MS Nutrition, DDS, FAAPD, DABPD, DAOS D entists are in a unique position to screen chil-dren for the recognizable signs and symptoms of mouth breathing, malocclusion, craniofa-cial anomalies and related conditions such as obstructive sleep apnea syndrome. 1 There is a lot of existing literature that shows that early orthodontic and orthopedic treatment impacts the airway and breathing. Orthodontic and orthopedic treatments that positively impact the airway and breathing can abso-lutely lead to a healthier and longer life for patients. Research studies have shown that airway obstruction impairs respiration. Impaired respiration can cause craniofacial malformation, malocclusion and jaw defor-mation. Research also shows that abnormal craniofacial formation can lead to airway obstruction, impaired respiration, impaired nasal breathing, chronic mouth breathing, sleep apnea, sleep disorders and lifelong ill-health. Early dental diagnosis and treatment of airway dysfunction and craniofacial malformation starting at birth is thus essential. Mouth breathing causes many muscles normally not used during respiration to be utilized. These recruited muscles become essential in maintaining the oral airway and they exert an atypical muscle tension on the facial bones. This action often leads to facial dishar-mony and malocclusion. 2 The airway, mode of breathing and craniofacial formation, are so inter-related during growth and devel-opment that form can follow function, and function can follow form. So, it is imperative to normalize form and function as early as possible, such that function is optimized for life. The growth of the face (excluding the mandible) is completed at a relatively early age. Sixty percent of craniofacial development takes place during the first four years of life and 90% by age 12. 3 Most formation and/or deformation occur by that age. Unfortunately, age 12 is still the average age that orthodontic and orthopedic treatment starts for most children world-wide. This should change. Early Diagnosis In order to better influence craniofacial growth and development, disparities must be recognized and addressed much earlier than at the current age of 12. More attention needs to be placed on routine cranio-facial examination, diagnosis and treatment beginning at birth. At the age of two and three, subtle dental signs of nasal obstruction and mouth breathing can be seen. Some of the clearest signs include open bite, posterior cross-bite and excessive over-jet. From ages three to twelve, early airway obstruction and craniofacial defor-mations quite often magnify themselves to such an extent that time inversely relates to the ease and options for correction. When obligate mouth breathing Fig. 1 36 Fall 2018 JAOS
Journal of the American Orthodontic Society Fall 2018: Page 36