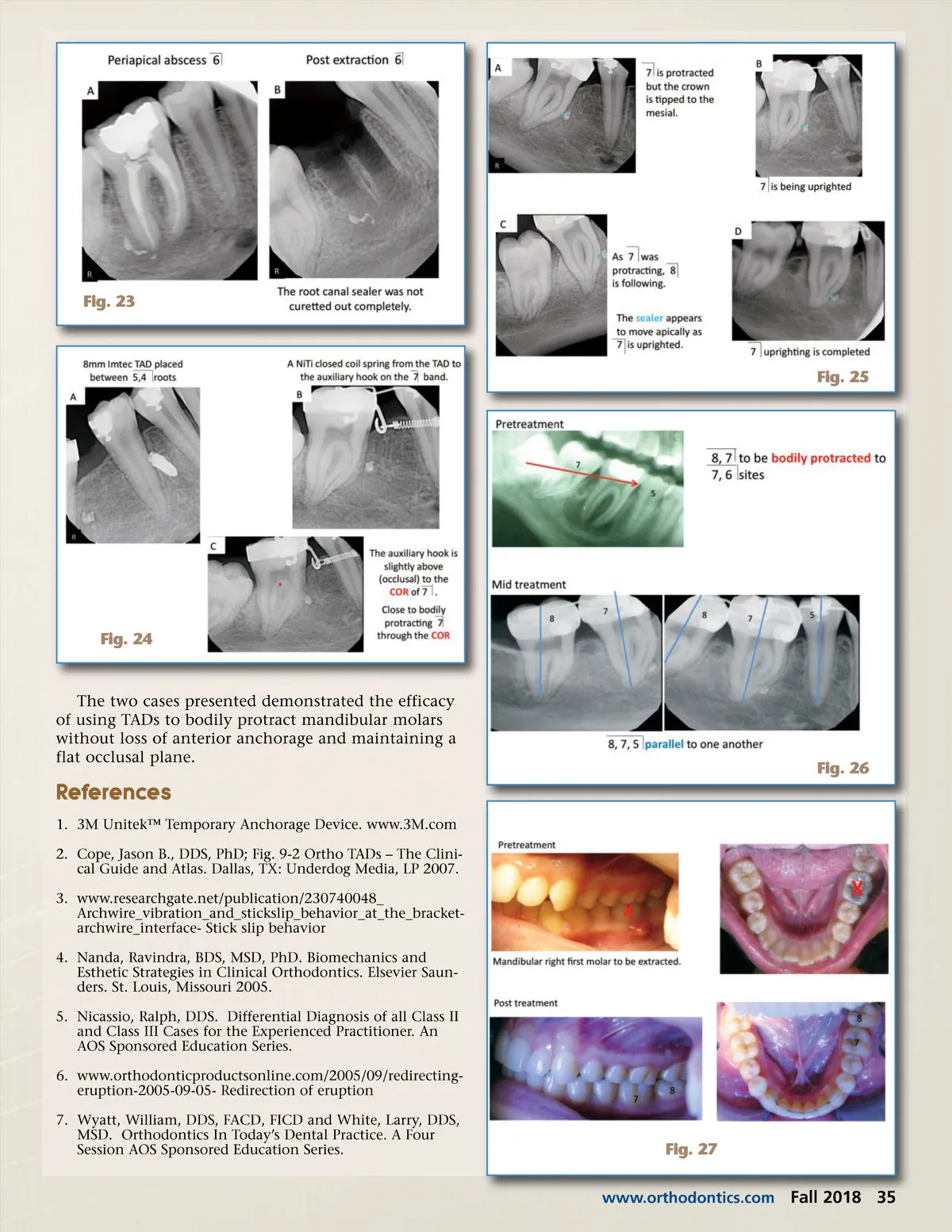
Fig. 21 Fig. 19 the mandibular second molars into the first molar sites (Fig. 20). The patient and her parents were very happy at the end of treatment (Fig. 21)! Case #2 This patient presented with an abscessed right mandibular first molar (Fig. 22). After root canal ther-apy performed by an endodontist, the tooth remained problematic and chronically infected. Upon inspec-tion, it appeared that the mesial canals were not obtu-rated to length (Fig. 23-A). Treatment options were presented, and the patient decided to have this tooth extracted (Fig. 23-B) and have the mandibular right second and third molars orthodontically protracted into the first and second molars sites. I extracted the mandibular right first molar and curetted the site, but inadvertently left a puff of sealer in the socket (Fig. 23-B). An 8 mm TAD was placed between the diverged roots of the mandibular bicuspids (Fig. 24-A). An auxiliary was fabricated and placed on the bracket assembly of the mandibular right second molar (Fig. 24-B). A 3 mm medium NiTi closed coil spring with eyelets was connected from the TAD to the auxiliary hook to protract the molar mesially (Fig. 24-B, C). The hook on the auxiliary was fabricated slightly occlusal to the COR of the mandibular right second molar due to a shallow vestibule (Fig. 25-C). The molar will protract, and the crown will rotate slightly to the mesial (Figs. 24-C, 25-A). After protraction of the mandibular first molar was completed (Fig. 25-A), final distal tipping of the crown was necessary. A distal tip bend was placed in the final archwire to tip the crown properly (Fig. 25-B, D). The sealer puff unintentionally left behind after extraction acted as a marker. As the tooth uprighted, the sealer appeared to move apically (Fig 25). Mid-treatment periapical radiographs of the mandibular second and third molars demonstrate proper crown position relative to their roots (Fig. 26). Post treatment illustrations show that the mandibular right second and third molars have been protracted and uprighted into the first and second molar sites (Fig. 27). Conclusion Traditional Type C space closure may be problem-atic. 4 Frictionless closure with closing loops may result in loss of anterior anchorage. Space closure using power chain (friction) may result in excessive tipping of the anterior and posterior teeth crowns and an uneven occlusal plane (Fig. 22). Fig. 20 Fig. 22 34 Fall 2018 JAOS
Journal of the American Orthodontic Society Fall 2018: Page 34