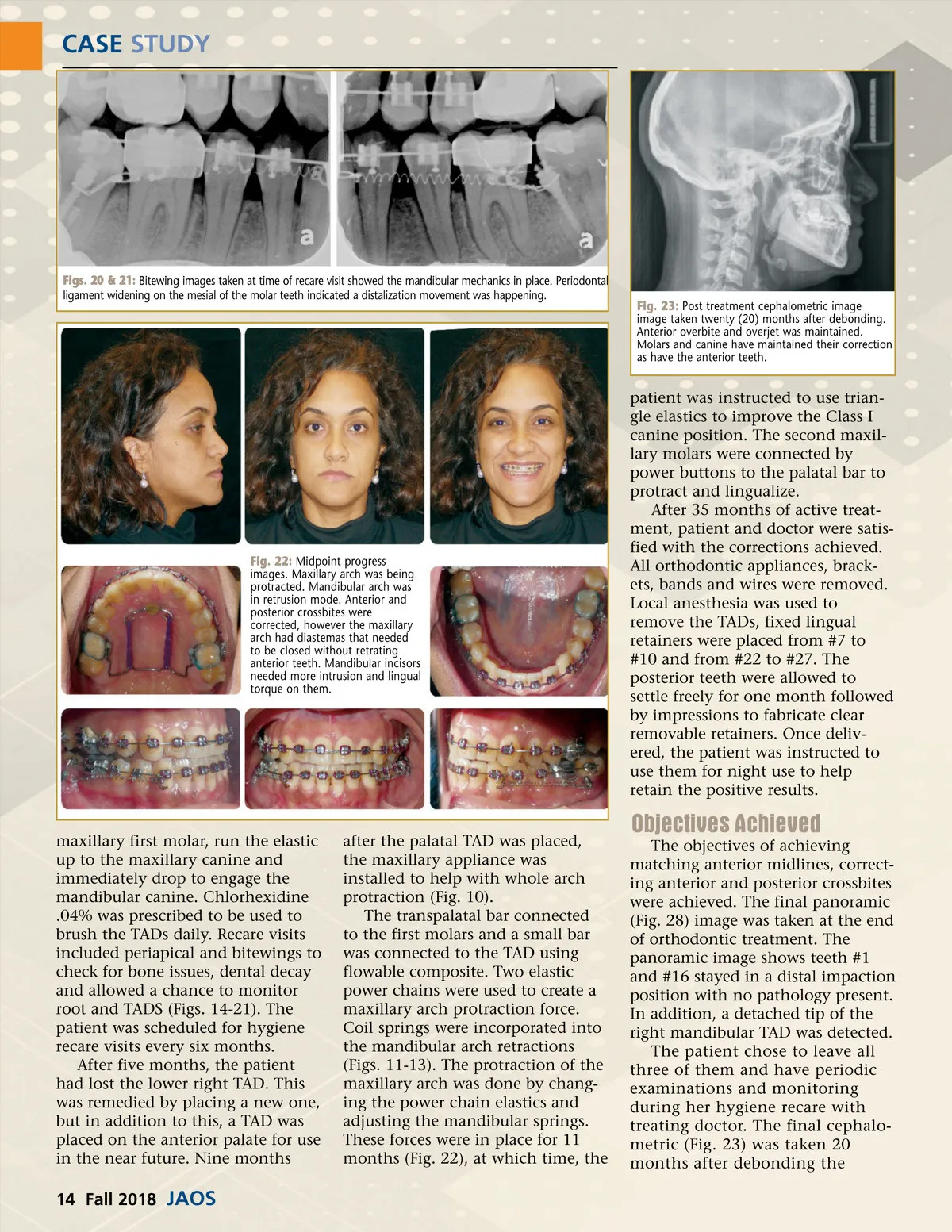
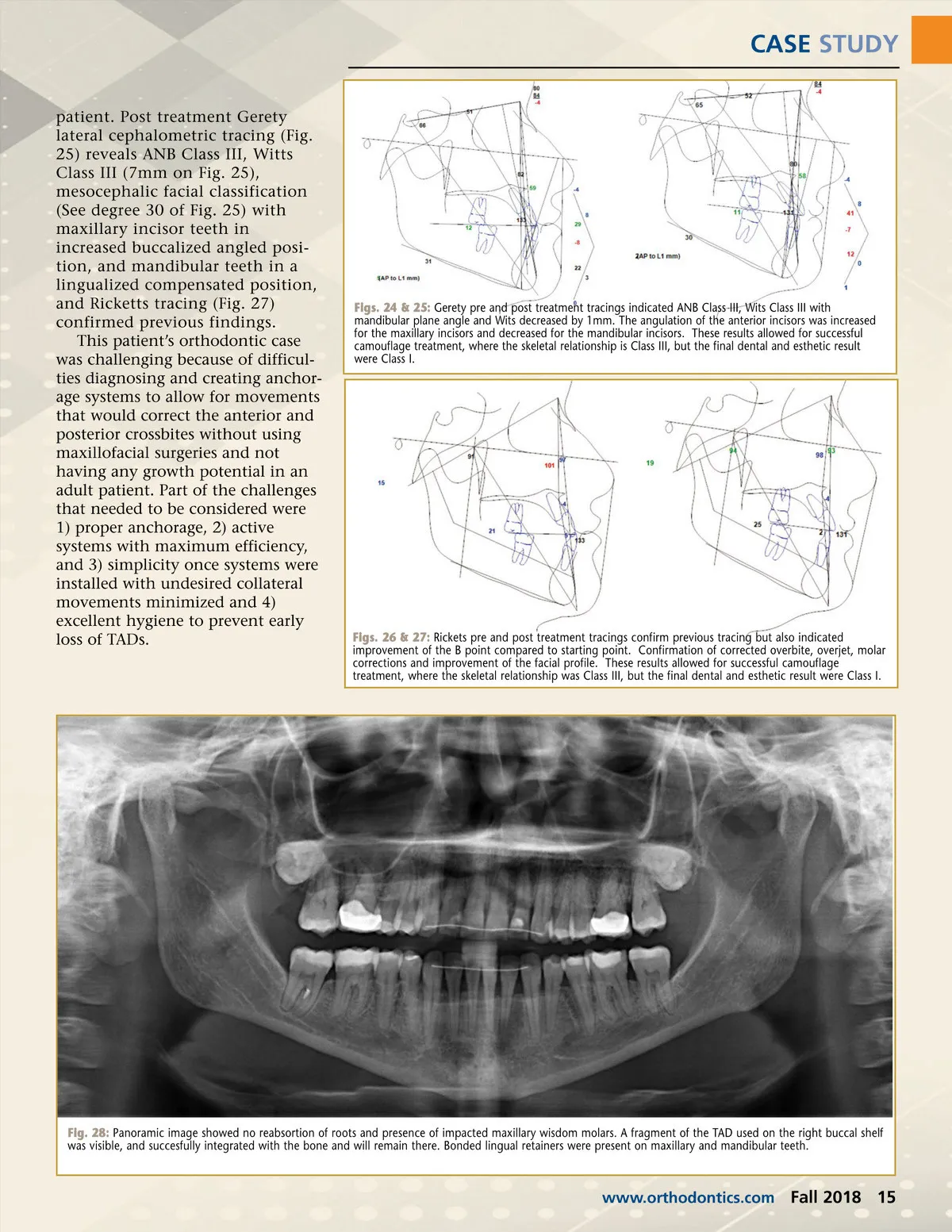
CASE STUDY Figs. 20 & 21: Bitewing images taken at time of recare visit showed the mandibular mechanics in place. Periodontal ligament widening on the mesial of the molar teeth indicated a distalization movement was happening. Fig. 23: Post treatment cephalometric image image taken twenty (20) months after debonding. Anterior overbite and overjet was maintained. Molars and canine have maintained their correction as have the anterior teeth. Fig. 22: Midpoint progress images. Maxillary arch was being protracted. Mandibular arch was in retrusion mode. Anterior and posterior crossbites were corrected, however the maxillary arch had diastemas that needed to be closed without retrating anterior teeth. Mandibular incisors needed more intrusion and lingual torque on them. patient was instructed to use trian-gle elastics to improve the Class I canine position. The second maxil-lary molars were connected by power buttons to the palatal bar to protract and lingualize. After 35 months of active treat-ment, patient and doctor were satis-fied with the corrections achieved. All orthodontic appliances, brack-ets, bands and wires were removed. Local anesthesia was used to remove the TADs, fixed lingual retainers were placed from #7 to #10 and from #22 to #27. The posterior teeth were allowed to settle freely for one month followed by impressions to fabricate clear removable retainers. Once deliv-ered, the patient was instructed to use them for night use to help retain the positive results. Objectives Achieved maxillary first molar, run the elastic up to the maxillary canine and immediately drop to engage the mandibular canine. Chlorhexidine .04% was prescribed to be used to brush the TADs daily. Recare visits included periapical and bitewings to check for bone issues, dental decay and allowed a chance to monitor root and TADS (Figs. 14-21). The patient was scheduled for hygiene recare visits every six months. After five months, the patient had lost the lower right TAD. This was remedied by placing a new one, but in addition to this, a TAD was placed on the anterior palate for use in the near future. Nine months after the palatal TAD was placed, the maxillary appliance was installed to help with whole arch protraction (Fig. 10). The transpalatal bar connected to the first molars and a small bar was connected to the TAD using flowable composite. Two elastic power chains were used to create a maxillary arch protraction force. Coil springs were incorporated into the mandibular arch retractions (Figs. 11-13). The protraction of the maxillary arch was done by chang-ing the power chain elastics and adjusting the mandibular springs. These forces were in place for 11 months (Fig. 22), at which time, the The objectives of achieving matching anterior midlines, correct-ing anterior and posterior crossbites were achieved. The final panoramic (Fig. 28) image was taken at the end of orthodontic treatment. The panoramic image shows teeth #1 and #16 stayed in a distal impaction position with no pathology present. In addition, a detached tip of the right mandibular TAD was detected. The patient chose to leave all three of them and have periodic examinations and monitoring during her hygiene recare with treating doctor. The final cephalo-metric (Fig. 23) was taken 20 months after debonding the 14 Fall 2018 JAOS
Journal of the American Orthodontic Society Fall 2018: Page 14