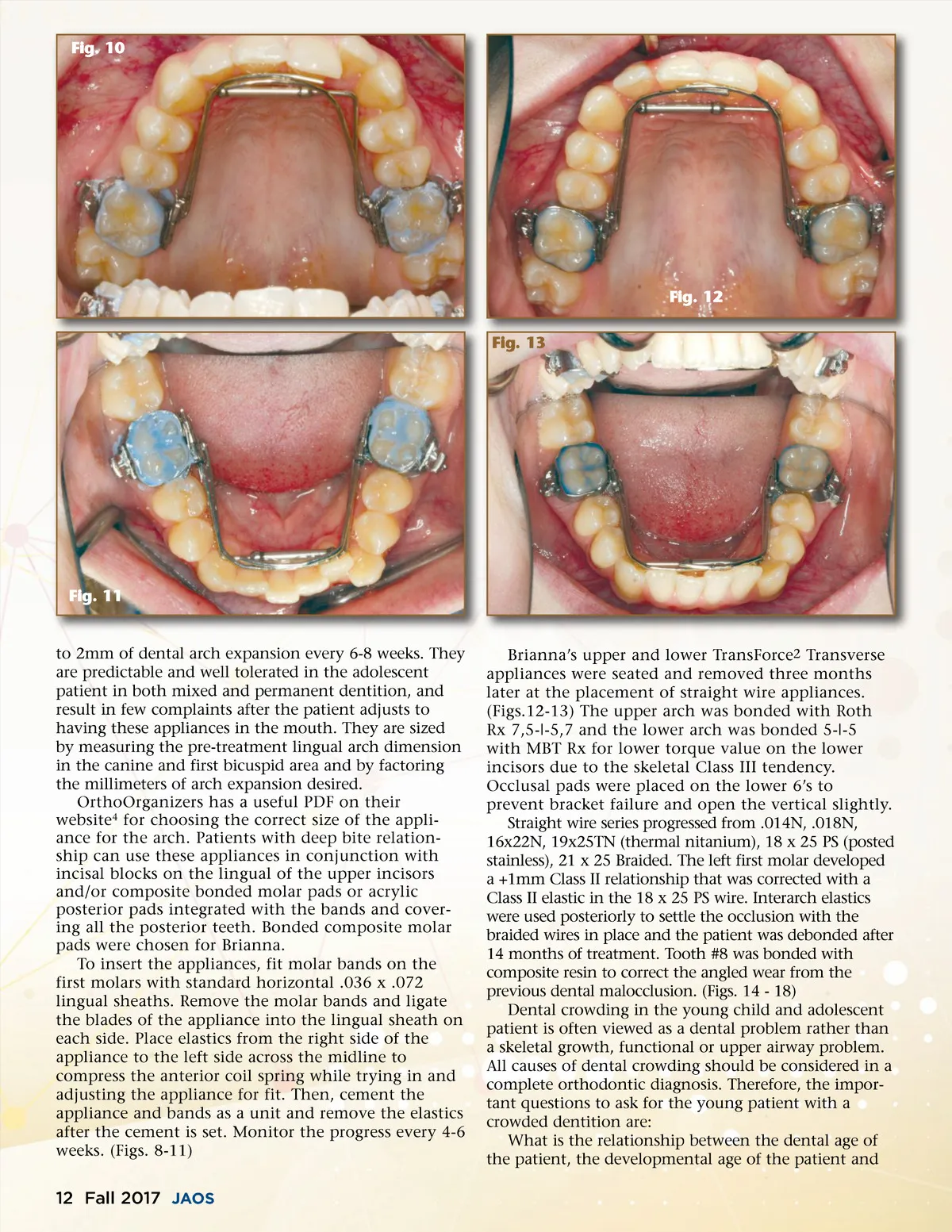
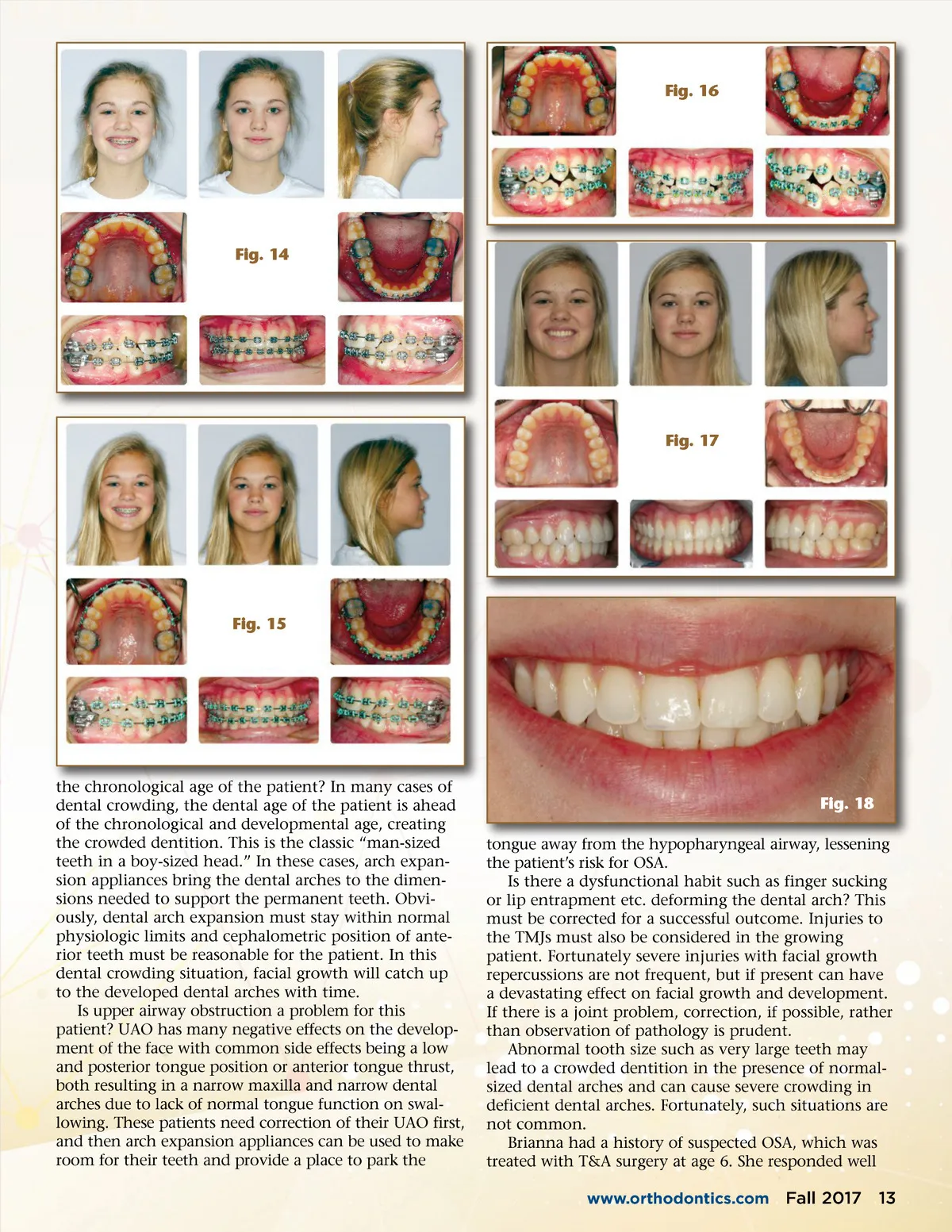
Fig. 10 Fig. 12 Fig. 13 Fig. 11 to 2mm of dental arch expansion every 6-8 weeks. They are predictable and well tolerated in the adolescent patient in both mixed and permanent dentition, and result in few complaints after the patient adjusts to having these appliances in the mouth. They are sized by measuring the pre-treatment lingual arch dimension in the canine and first bicuspid area and by factoring the millimeters of arch expansion desired. OrthoOrganizers has a useful PDF on their website 4 for choosing the correct size of the appli-ance for the arch. Patients with deep bite relation-ship can use these appliances in conjunction with incisal blocks on the lingual of the upper incisors and/or composite bonded molar pads or acrylic posterior pads integrated with the bands and cover-ing all the posterior teeth. Bonded composite molar pads were chosen for Brianna. To insert the appliances, fit molar bands on the first molars with standard horizontal .036 x .072 lingual sheaths. Remove the molar bands and ligate the blades of the appliance into the lingual sheath on each side. Place elastics from the right side of the appliance to the left side across the midline to compress the anterior coil spring while trying in and adjusting the appliance for fit. Then, cement the appliance and bands as a unit and remove the elastics after the cement is set. Monitor the progress every 4-6 weeks. (Figs. 8-11) Brianna’s upper and lower TransForce 2 Transverse appliances were seated and removed three months later at the placement of straight wire appliances. (Figs.12-13) The upper arch was bonded with Roth Rx 7,5-|-5,7 and the lower arch was bonded 5-|-5 with MBT Rx for lower torque value on the lower incisors due to the skeletal Class III tendency. Occlusal pads were placed on the lower 6’s to prevent bracket failure and open the vertical slightly. Straight wire series progressed from .014N, .018N, 16x22N, 19x25TN (thermal nitanium), 18 x 25 PS (posted stainless), 21 x 25 Braided. The left first molar developed a +1mm Class II relationship that was corrected with a Class II elastic in the 18 x 25 PS wire. Interarch elastics were used posteriorly to settle the occlusion with the braided wires in place and the patient was debonded after 14 months of treatment. Tooth #8 was bonded with composite resin to correct the angled wear from the previous dental malocclusion. (Figs. 14 -18) Dental crowding in the young child and adolescent patient is often viewed as a dental problem rather than a skeletal growth, functional or upper airway problem. All causes of dental crowding should be considered in a complete orthodontic diagnosis. Therefore, the impor-tant questions to ask for the young patient with a crowded dentition are: What is the relationship between the dental age of the patient, the developmental age of the patient and 12 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 12