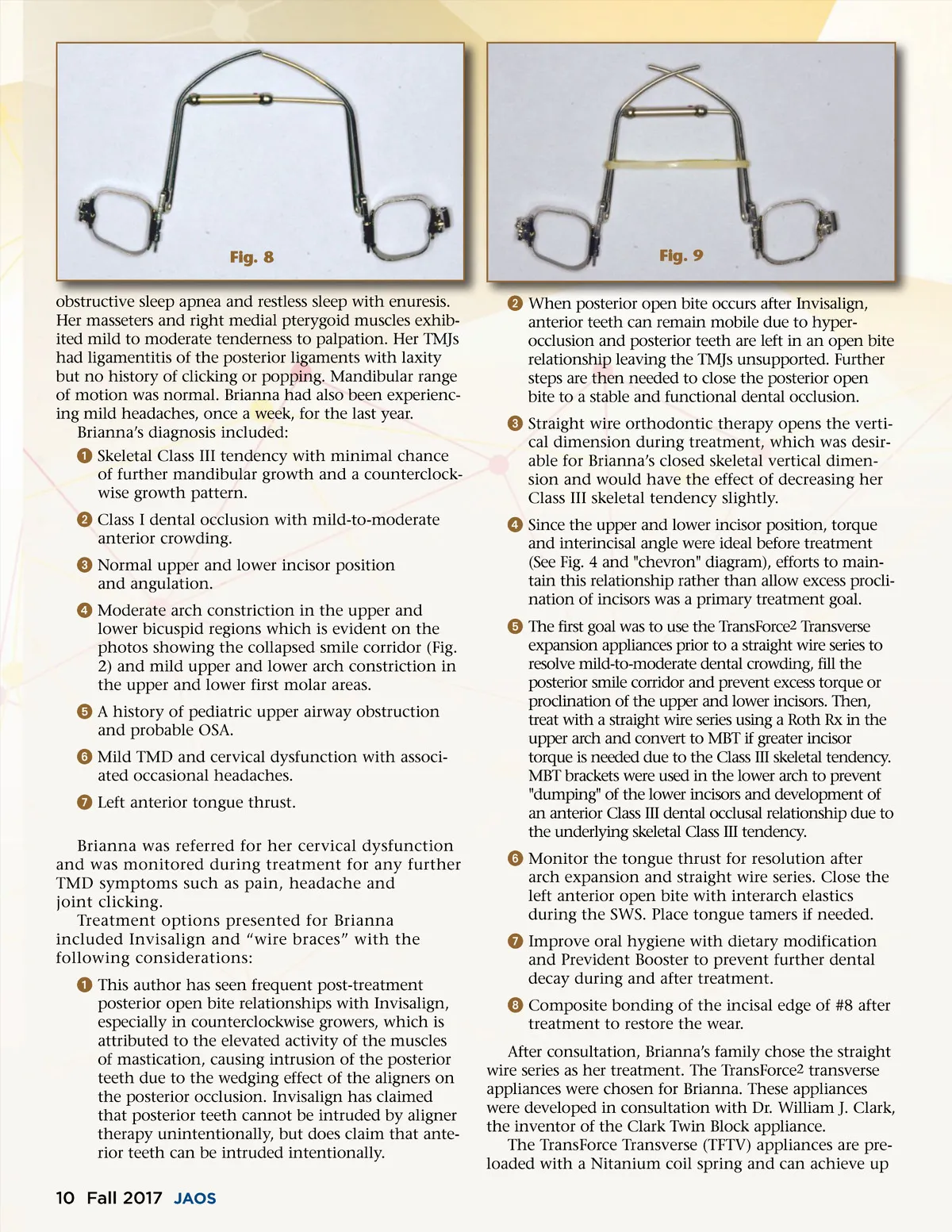
Fig. 8 obstructive sleep apnea and restless sleep with enuresis. Her masseters and right medial pterygoid muscles exhib-ited mild to moderate tenderness to palpation. Her TMJs had ligamentitis of the posterior ligaments with laxity but no history of clicking or popping. Mandibular range of motion was normal. Brianna had also been experienc-ing mild headaches, once a week, for the last year. Brianna’s diagnosis included: ᕡ Skeletal Class III tendency with minimal chance of further mandibular growth and a counterclock-wise growth pattern. ᕢ Class I dental occlusion with mild-to-moderate anterior crowding. ᕣ Normal upper and lower incisor position and angulation. ᕤ Moderate arch constriction in the upper and lower bicuspid regions which is evident on the photos showing the collapsed smile corridor (Fig. 2) and mild upper and lower arch constriction in the upper and lower first molar areas. ᕥ A history of pediatric upper airway obstruction and probable OSA. ᕦ Mild TMD and cervical dysfunction with associ-ated occasional headaches. ᕧ Left anterior tongue thrust. Brianna was referred for her cervical dysfunction and was monitored during treatment for any further TMD symptoms such as pain, headache and joint clicking. Treatment options presented for Brianna included Invisalign and “wire braces” with the following considerations: ᕡ This author has seen frequent post-treatment posterior open bite relationships with Invisalign, especially in counterclockwise growers, which is attributed to the elevated activity of the muscles of mastication, causing intrusion of the posterior teeth due to the wedging effect of the aligners on the posterior occlusion. Invisalign has claimed that posterior teeth cannot be intruded by aligner therapy unintentionally, but does claim that ante-rior teeth can be intruded intentionally. Fig. 9 ᕢ When posterior open bite occurs after Invisalign, anterior teeth can remain mobile due to hyper-occlusion and posterior teeth are left in an open bite relationship leaving the TMJs unsupported. Further steps are then needed to close the posterior open bite to a stable and functional dental occlusion. ᕣ Straight wire orthodontic therapy opens the verti-cal dimension during treatment, which was desir-able for Brianna’s closed skeletal vertical dimen-sion and would have the effect of decreasing her Class III skeletal tendency slightly. ᕤ Since the upper and lower incisor position, torque and interincisal angle were ideal before treatment (See Fig. 4 and "chevron" diagram), efforts to main-tain this relationship rather than allow excess procli-nation of incisors was a primary treatment goal. ᕥ The first goal was to use the TransForce 2 Transverse expansion appliances prior to a straight wire series to resolve mild-to-moderate dental crowding, fill the posterior smile corridor and prevent excess torque or proclination of the upper and lower incisors. Then, treat with a straight wire series using a Roth Rx in the upper arch and convert to MBT if greater incisor torque is needed due to the Class III skeletal tendency. MBT brackets were used in the lower arch to prevent "dumping" of the lower incisors and development of an anterior Class III dental occlusal relationship due to the underlying skeletal Class III tendency. ᕦ Monitor the tongue thrust for resolution after arch expansion and straight wire series. Close the left anterior open bite with interarch elastics during the SWS. Place tongue tamers if needed. ᕧ Improve oral hygiene with dietary modification and Prevident Booster to prevent further dental decay during and after treatment. ᕨ Composite bonding of the incisal edge of #8 after treatment to restore the wear. After consultation, Brianna’s family chose the straight wire series as her treatment. The TransForce 2 transverse appliances were chosen for Brianna. These appliances were developed in consultation with Dr. William J. Clark, the inventor of the Clark Twin Block appliance. The TransForce Transverse (TFTV) appliances are pre-loaded with a Nitanium coil spring and can achieve up 10 Fall 2017 JAOS
Journal of the American Orthodontic Society Fall 2017: Page 10