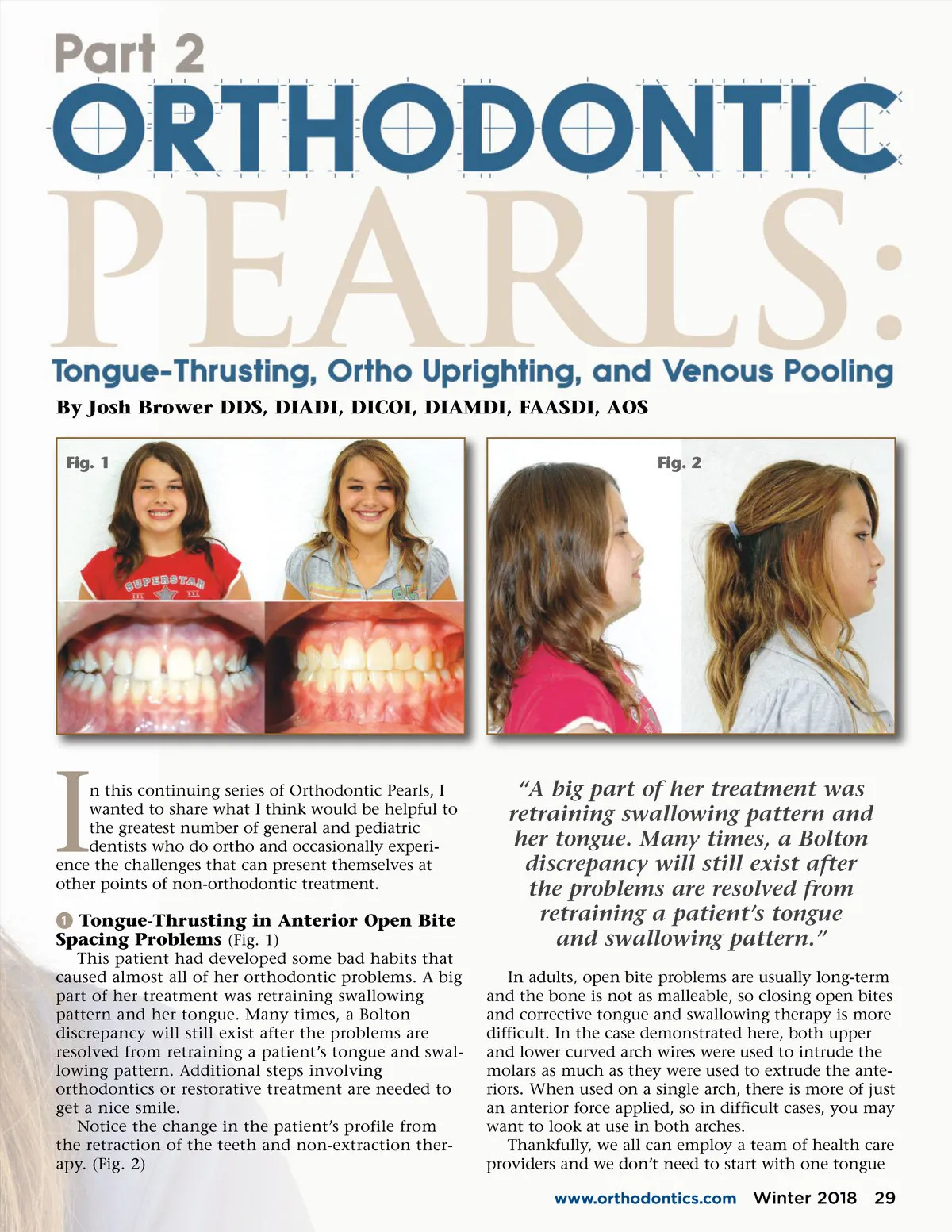
By Josh Brower DDS, DIADI, DICOI, DIAMDI, FAASDI, AOS Fig. 1 Fig. 2 I n this continuing series of Orthodontic Pearls, I wanted to share what I think would be helpful to the greatest number of general and pediatric dentists who do ortho and occasionally experi-ence the challenges that can present themselves at other points of non-orthodontic treatment. ᕡ Tongue-Thrusting in Anterior Open Bite Spacing Problems (Fig. 1) This patient had developed some bad habits that caused almost all of her orthodontic problems. A big part of her treatment was retraining swallowing pattern and her tongue. Many times, a Bolton discrepancy will still exist after the problems are resolved from retraining a patient’s tongue and swal-lowing pattern. Additional steps involving orthodontics or restorative treatment are needed to get a nice smile. Notice the change in the patient’s profile from the retraction of the teeth and non-extraction ther-apy. (Fig. 2) “A big part of her treatment was retraining swallowing pattern and her tongue. Many times, a Bolton discrepancy will still exist after the problems are resolved from retraining a patient’s tongue and swallowing pattern.” In adults, open bite problems are usually long-term and the bone is not as malleable, so closing open bites and corrective tongue and swallowing therapy is more difficult. In the case demonstrated here, both upper and lower curved arch wires were used to intrude the molars as much as they were used to extrude the ante-riors. When used on a single arch, there is more of just an anterior force applied, so in difficult cases, you may want to look at use in both arches. Thankfully, we all can employ a team of health care providers and we don’t need to start with one tongue www.orthodontics.com Winter 2018 29
Journal of the American Orthodontic Society Winter 2018: Page 29