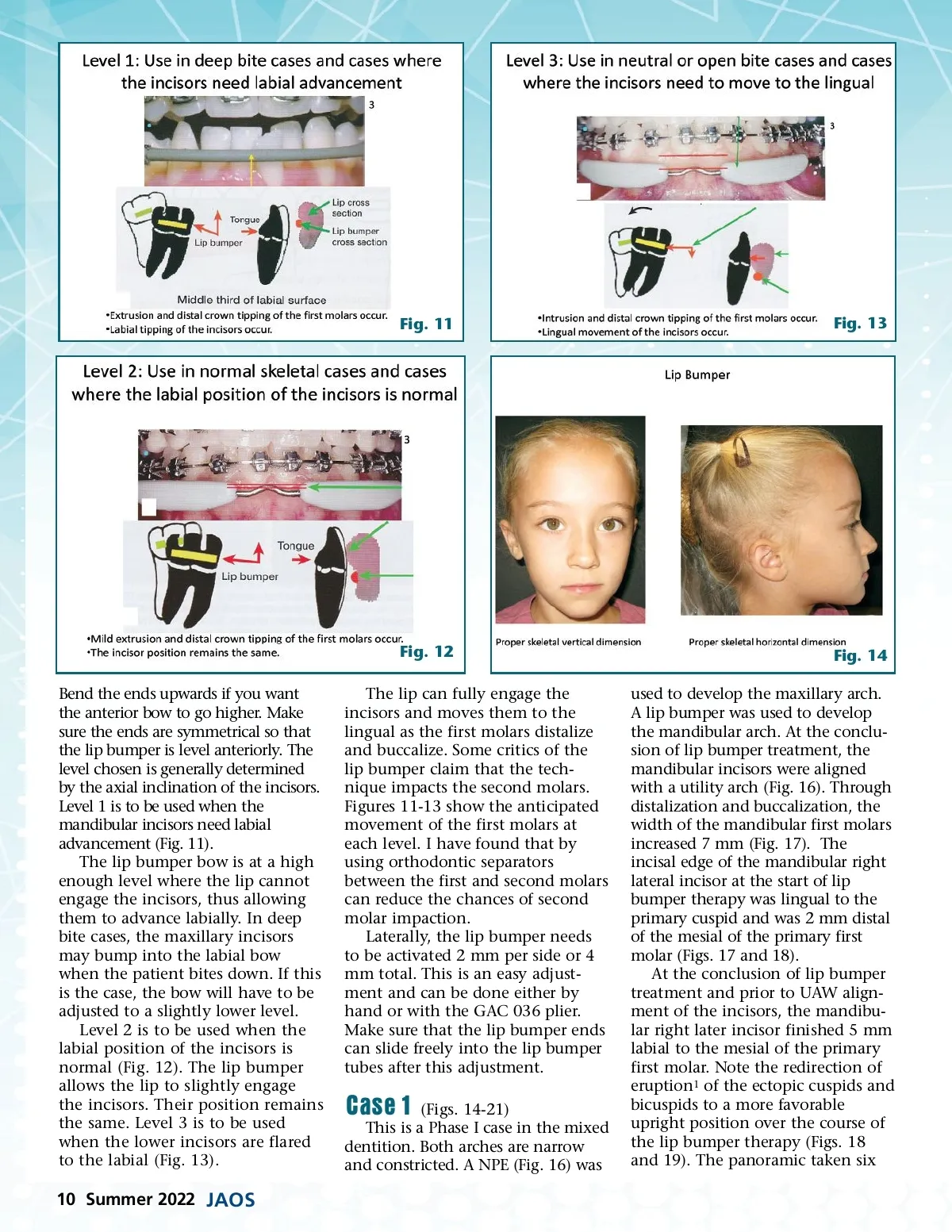
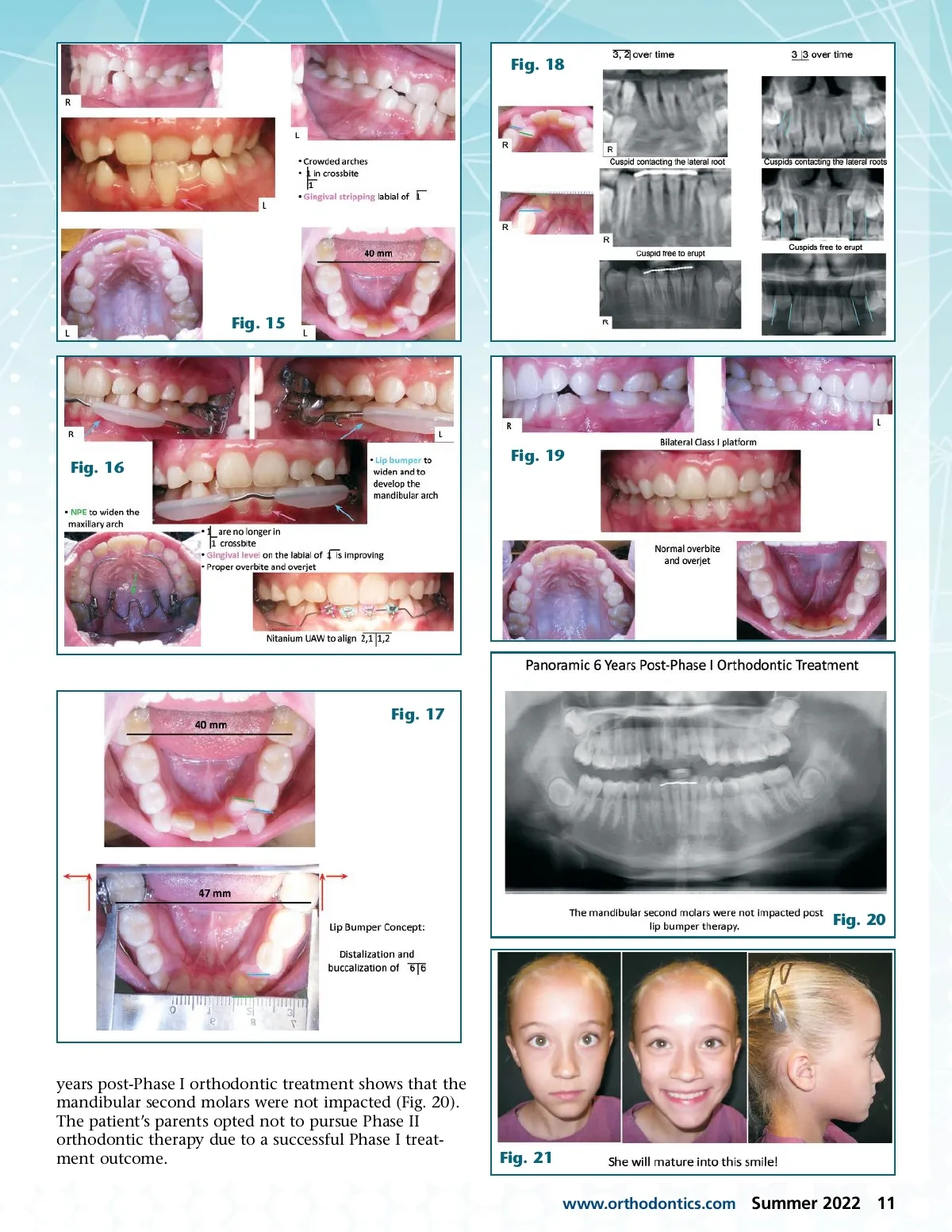
Fig. 11 Fig. 13 Fig. 12 Bend the ends upwards if you want the anterior bow to go higher. Make sure the ends are symmetrical so that the lip bumper is level anteriorly. The level chosen is generally determined by the axial inclination of the incisors. Level 1 is to be used when the mandibular incisors need labial advancement (Fig. 11). The lip bumper bow is at a high enough level where the lip cannot engage the incisors, thus allowing them to advance labially. In deep bite cases, the maxillary incisors may bump into the labial bow when the patient bites down. If this is the case, the bow will have to be adjusted to a slightly lower level. Level 2 is to be used when the labial position of the incisors is normal (Fig. 12). The lip bumper allows the lip to slightly engage the incisors. Their position remains the same. Level 3 is to be used when the lower incisors are flared to the labial (Fig. 13). The lip can fully engage the incisors and moves them to the lingual as the first molars distalize and buccalize. Some critics of the lip bumper claim that the tech-nique impacts the second molars. Figures 11-13 show the anticipated movement of the first molars at each level. I have found that by using orthodontic separators between the first and second molars can reduce the chances of second molar impaction. Laterally, the lip bumper needs to be activated 2 mm per side or 4 mm total. This is an easy adjust-ment and can be done either by hand or with the GAC 036 plier. Make sure that the lip bumper ends can slide freely into the lip bumper tubes after this adjustment. Fig. 14 used to develop the maxillary arch. A lip bumper was used to develop the mandibular arch. At the conclu-sion of lip bumper treatment, the mandibular incisors were aligned with a utility arch (Fig. 16). Through distalization and buccalization, the width of the mandibular first molars increased 7 mm (Fig. 17). The incisal edge of the mandibular right lateral incisor at the start of lip bumper therapy was lingual to the primary cuspid and was 2 mm distal of the mesial of the primary first molar (Figs. 17 and 18). At the conclusion of lip bumper treatment and prior to UAW align-ment of the incisors, the mandibu-lar right later incisor finished 5 mm labial to the mesial of the primary first molar. Note the redirection of eruption 1 of the ectopic cuspids and bicuspids to a more favorable upright position over the course of the lip bumper therapy (Figs. 18 and 19). The panoramic taken six Case 1 (Figs. 14-21) This is a Phase I case in the mixed dentition. Both arches are narrow and constricted. A NPE (Fig. 16) was 10 Summer 2022 JAOS
Journal of the American Orthodontic Society Summer 2022: Page 10