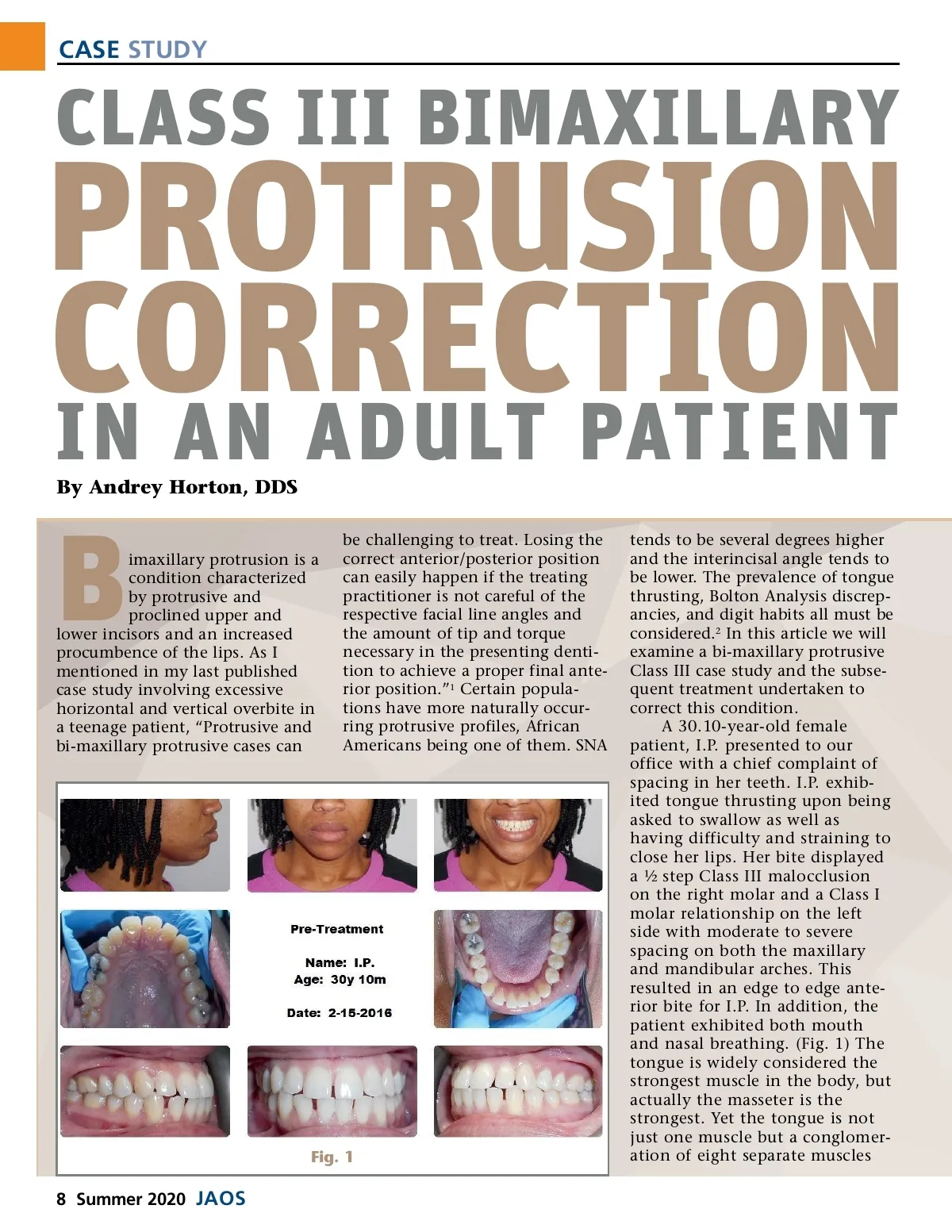
CASE STUDY CLASS III BIMAXILLARY PROTRUSION CORRECTION IN AN ADULT PATIENT By Andrey Horton, DDS imaxillary protrusion is a condition characterized by protrusive and proclined upper and lower incisors and an increased procumbence of the lips. As I mentioned in my last published case study involving excessive horizontal and vertical overbite in a teenage patient, “Protrusive and bi-maxillary protrusive cases can B be challenging to treat. Losing the correct anterior/posterior position can easily happen if the treating practitioner is not careful of the respective facial line angles and the amount of tip and torque necessary in the presenting denti-tion to achieve a proper final ante-rior position.” 1 Certain popula-tions have more naturally occur-ring protrusive profiles, African Americans being one of them. SNA Fig. 1 tends to be several degrees higher and the interincisal angle tends to be lower. The prevalence of tongue thrusting, Bolton Analysis discrep-ancies, and digit habits all must be considered. 2 In this article we will examine a bi-maxillary protrusive Class III case study and the subse-quent treatment undertaken to correct this condition. A 30.10-year-old female patient, I.P. presented to our office with a chief complaint of spacing in her teeth. I.P. exhib-ited tongue thrusting upon being asked to swallow as well as having difficulty and straining to close her lips. Her bite displayed a ½ step Class III malocclusion on the right molar and a Class I molar relationship on the left side with moderate to severe spacing on both the maxillary and mandibular arches. This resulted in an edge to edge ante-rior bite for I.P. In addition, the patient exhibited both mouth and nasal breathing. (Fig. 1) The tongue is widely considered the strongest muscle in the body, but actually the masseter is the strongest. Yet the tongue is not just one muscle but a conglomer-ation of eight separate muscles 8 Summer 2020 JAOS
Journal of the American Orthodontic Society Summer 2020: Page 8