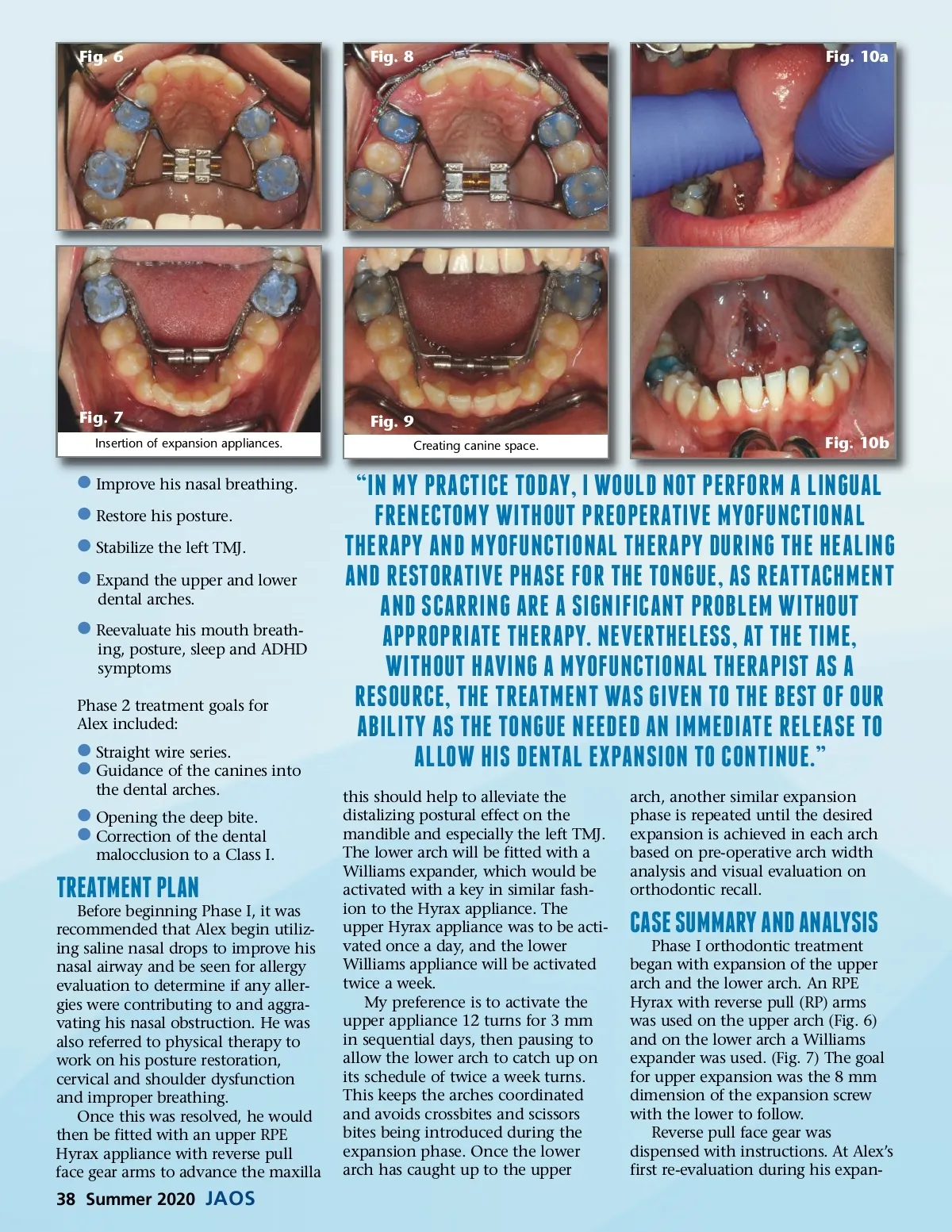
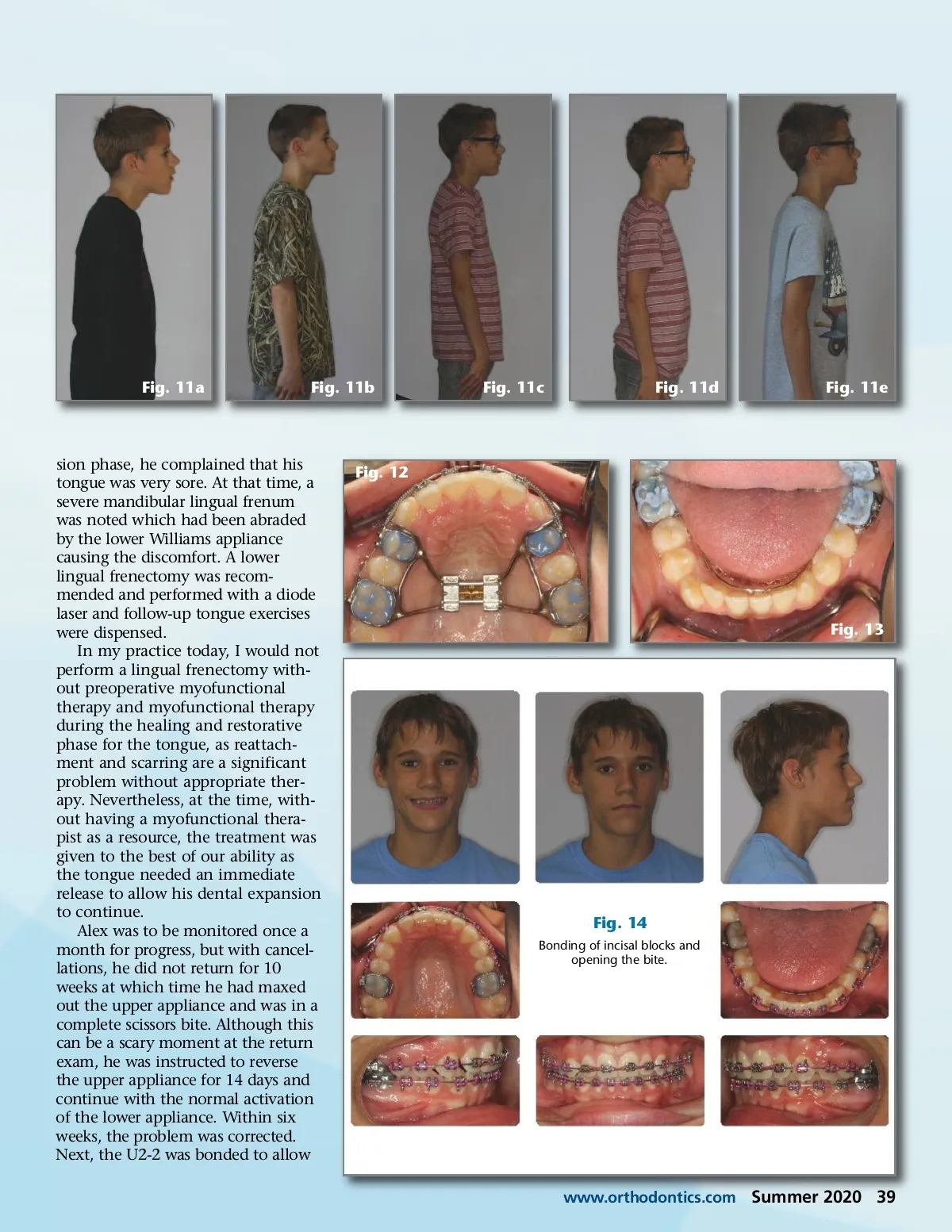
Fig. 11a Fig. 11b Fig. 11c Fig. 11d Fig. 11e sion phase, he complained that his tongue was very sore. At that time, a severe mandibular lingual frenum was noted which had been abraded by the lower Williams appliance causing the discomfort. A lower lingual frenectomy was recom-mended and performed with a diode laser and follow-up tongue exercises were dispensed. In my practice today, I would not perform a lingual frenectomy with-out preoperative myofunctional therapy and myofunctional therapy during the healing and restorative phase for the tongue, as reattach-ment and scarring are a significant problem without appropriate ther-apy. Nevertheless, at the time, with-out having a myofunctional thera-pist as a resource, the treatment was given to the best of our ability as the tongue needed an immediate release to allow his dental expansion to continue. Alex was to be monitored once a month for progress, but with cancel-lations, he did not return for 10 weeks at which time he had maxed out the upper appliance and was in a complete scissors bite. Although this can be a scary moment at the return exam, he was instructed to reverse the upper appliance for 14 days and continue with the normal activation of the lower appliance. Within six weeks, the problem was corrected. Next, the U2-2 was bonded to allow Fig. 12 Fig. 13 Fig. 14 Bonding of incisal blocks and opening the bite. www.orthodontics.com Summer 2020 39
Journal of the American Orthodontic Society Summer 2020: Page 39