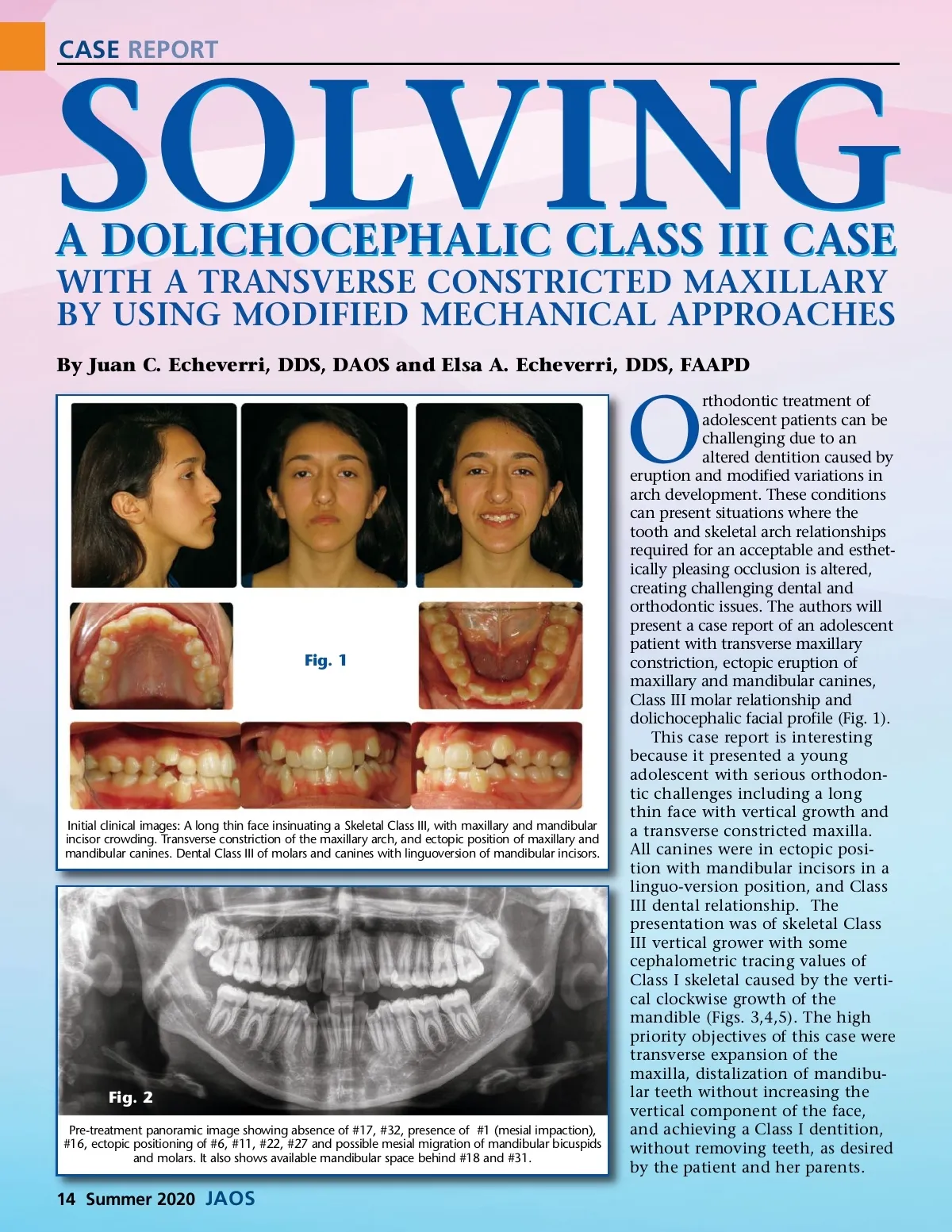
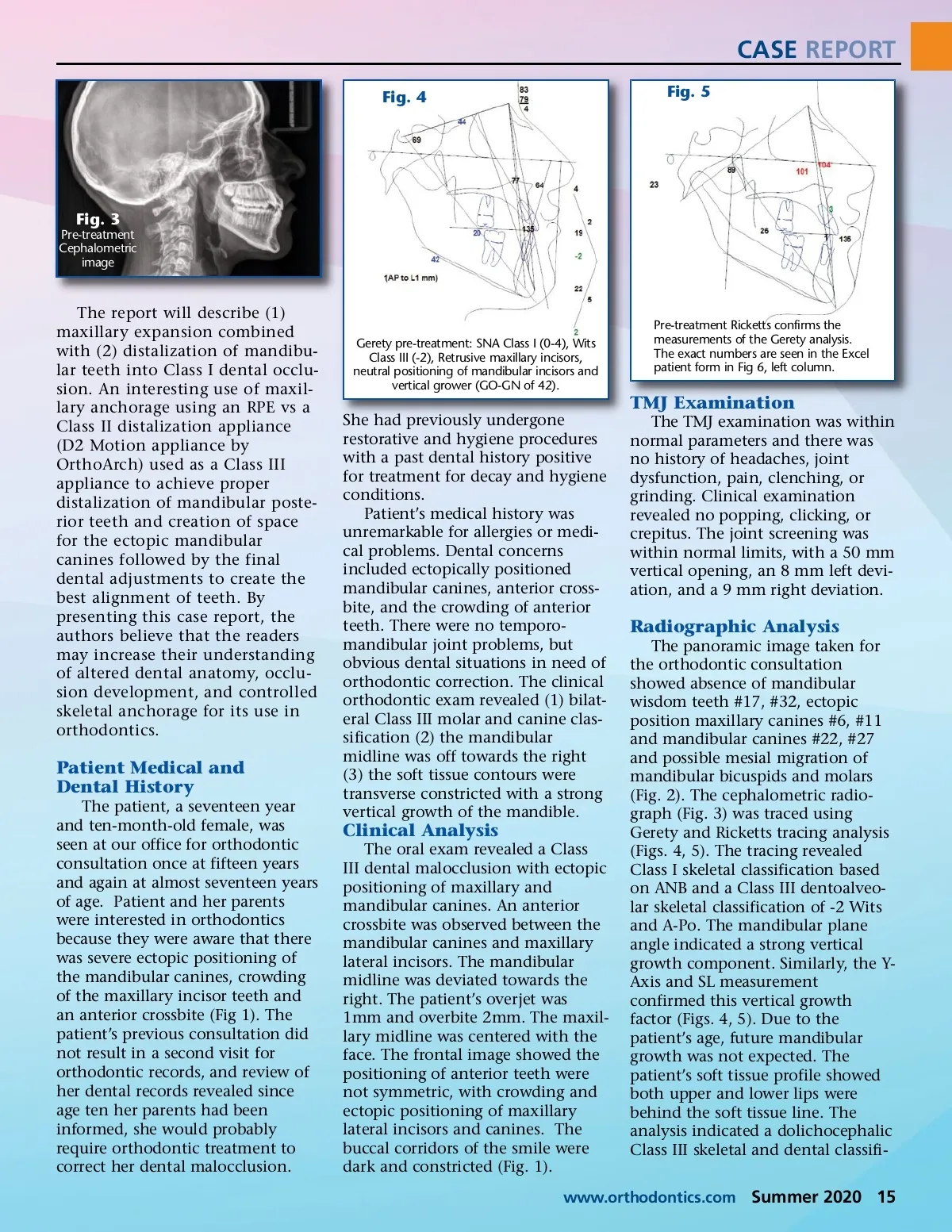
CASE REPORT Fig. 4 Fig. 5 Fig. 3 Pre-treatment Cephalometric image The report will describe (1) maxillary expansion combined with (2) distalization of mandibu-lar teeth into Class I dental occlu-sion. An interesting use of maxil-lary anchorage using an RPE vs a Class II distalization appliance (D2 Motion appliance by OrthoArch) used as a Class III appliance to achieve proper distalization of mandibular poste-rior teeth and creation of space for the ectopic mandibular canines followed by the final dental adjustments to create the best alignment of teeth. By presenting this case report, the authors believe that the readers may increase their understanding of altered dental anatomy, occlu-sion development, and controlled skeletal anchorage for its use in orthodontics. Gerety pre-treatment: SNA Class I (0-4), Wits Class III (-2), Retrusive maxillary incisors, neutral positioning of mandibular incisors and vertical grower (GO-GN of 42). Pre-treatment Ricketts confirms the measurements of the Gerety analysis. The exact numbers are seen in the Excel patient form in Fig 6, left column. TMJ Examination She had previously undergone restorative and hygiene procedures with a past dental history positive for treatment for decay and hygiene conditions. Patient’s medical history was unremarkable for allergies or medi-cal problems. Dental concerns included ectopically positioned mandibular canines, anterior cross-bite, and the crowding of anterior teeth. There were no temporo-mandibular joint problems, but obvious dental situations in need of orthodontic correction. The clinical orthodontic exam revealed (1) bilat-eral Class III molar and canine clas-sification (2) the mandibular midline was off towards the right (3) the soft tissue contours were transverse constricted with a strong vertical growth of the mandible. The TMJ examination was within normal parameters and there was no history of headaches, joint dysfunction, pain, clenching, or grinding. Clinical examination revealed no popping, clicking, or crepitus. The joint screening was within normal limits, with a 50 mm vertical opening, an 8 mm left devi-ation, and a 9 mm right deviation. Radiographic Analysis The panoramic image taken for the orthodontic consultation showed absence of mandibular wisdom teeth #17, #32, ectopic position maxillary canines #6, #11 and mandibular canines #22, #27 and possible mesial migration of mandibular bicuspids and molars (Fig. 2). The cephalometric radio-graph (Fig. 3) was traced using Gerety and Ricketts tracing analysis (Figs. 4, 5). The tracing revealed Class I skeletal classification based on ANB and a Class III dentoalveo-lar skeletal classification of -2 Wits and A-Po. The mandibular plane angle indicated a strong vertical growth component. Similarly, the Y-Axis and SL measurement confirmed this vertical growth factor (Figs. 4, 5). Due to the patient’s age, future mandibular growth was not expected. The patient’s soft tissue profile showed both upper and lower lips were behind the soft tissue line. The analysis indicated a dolichocephalic Class III skeletal and dental classifi-Patient Medical and Dental History The patient, a seventeen year and ten-month-old female, was seen at our office for orthodontic consultation once at fifteen years and again at almost seventeen years of age. Patient and her parents were interested in orthodontics because they were aware that there was severe ectopic positioning of the mandibular canines, crowding of the maxillary incisor teeth and an anterior crossbite (Fig 1). The patient’s previous consultation did not result in a second visit for orthodontic records, and review of her dental records revealed since age ten her parents had been informed, she would probably require orthodontic treatment to correct her dental malocclusion. Clinical Analysis The oral exam revealed a Class III dental malocclusion with ectopic positioning of maxillary and mandibular canines. An anterior crossbite was observed between the mandibular canines and maxillary lateral incisors. The mandibular midline was deviated towards the right. The patient’s overjet was 1mm and overbite 2mm. The maxil-lary midline was centered with the face. The frontal image showed the positioning of anterior teeth were not symmetric, with crowding and ectopic positioning of maxillary lateral incisors and canines. The buccal corridors of the smile were dark and constricted (Fig. 1). www.orthodontics.com Summer 2020 15
Journal of the American Orthodontic Society Summer 2020: Page 15