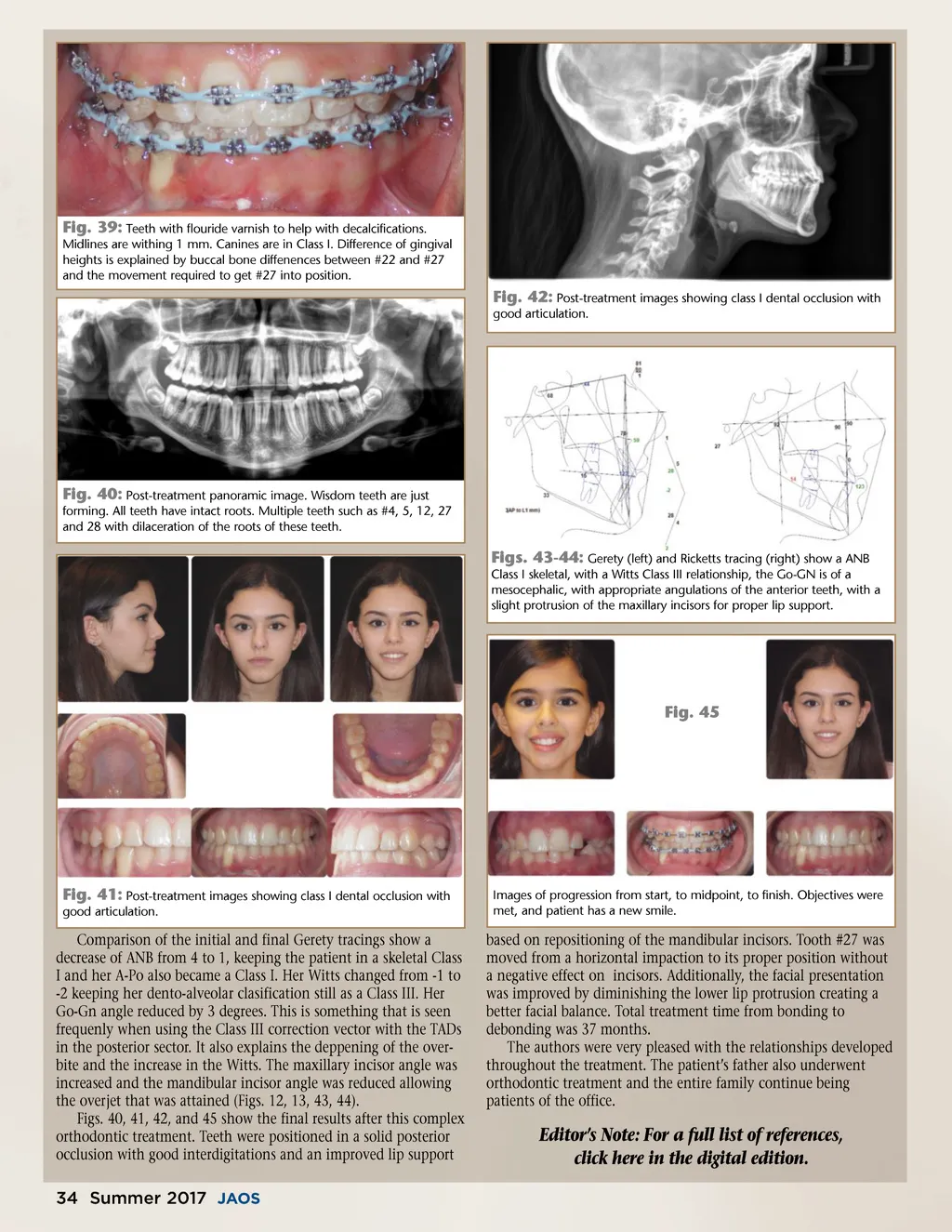
Fig. 39: Teeth with flouride varnish to help with decalcifications. Midlines are withing 1 mm. Canines are in Class I. Difference of gingival heights is explained by buccal bone diffenences between #22 and #27 and the movement required to get #27 into position. Fig. 42: Post-treatment images showing class I dental occlusion with good articulation. Fig. 40: Post-treatment panoramic image. Wisdom teeth are just forming. All teeth have intact roots. Multiple teeth such as #4, 5, 12, 27 and 28 with dilaceration of the roots of these teeth. Figs. 43-44: Gerety (left) and Ricketts tracing (right) show a ANB Class I skeletal, with a Witts Class III relationship, the Go-GN is of a mesocephalic, with appropriate angulations of the anterior teeth, with a slight protrusion of the maxillary incisors for proper lip support. Fig. 45 Fig. 41: Post-treatment images showing class I dental occlusion with good articulation. Comparison of the initial and final Gerety tracings show a decrease of ANB from 4 to 1, keeping the patient in a skeletal Class I and her A-Po also became a Class I. Her Witts changed from -1 to -2 keeping her dento-alveolar clasification still as a Class III. Her Go-Gn angle reduced by 3 degrees. This is something that is seen frequenly when using the Class III correction vector with the TADs in the posterior sector. It also explains the deppening of the over-bite and the increase in the Witts. The maxillary incisor angle was increased and the mandibular incisor angle was reduced allowing the overjet that was attained (Figs. 12, 13, 43, 44). Figs. 40, 41, 42, and 45 show the final results after this complex orthodontic treatment. Teeth were positioned in a solid posterior occlusion with good interdigitations and an improved lip support Images of progression from start, to midpoint, to finish. Objectives were met, and patient has a new smile. based on repositioning of the mandibular incisors. Tooth #27 was moved from a horizontal impaction to its proper position without a negative effect on incisors. Additionally, the facial presentation was improved by diminishing the lower lip protrusion creating a better facial balance. Total treatment time from bonding to debonding was 37 months. The authors were very pleased with the relationships developed throughout the treatment. The patient’s father also underwent orthodontic treatment and the entire family continue being patients of the office. Editor’s Note: For a full list of references, click here in the digital edition. 34 Summer 2017 JAOS
Journal of the American Orthodontic Society Summer 2017/Buyer's Guide: Page 34