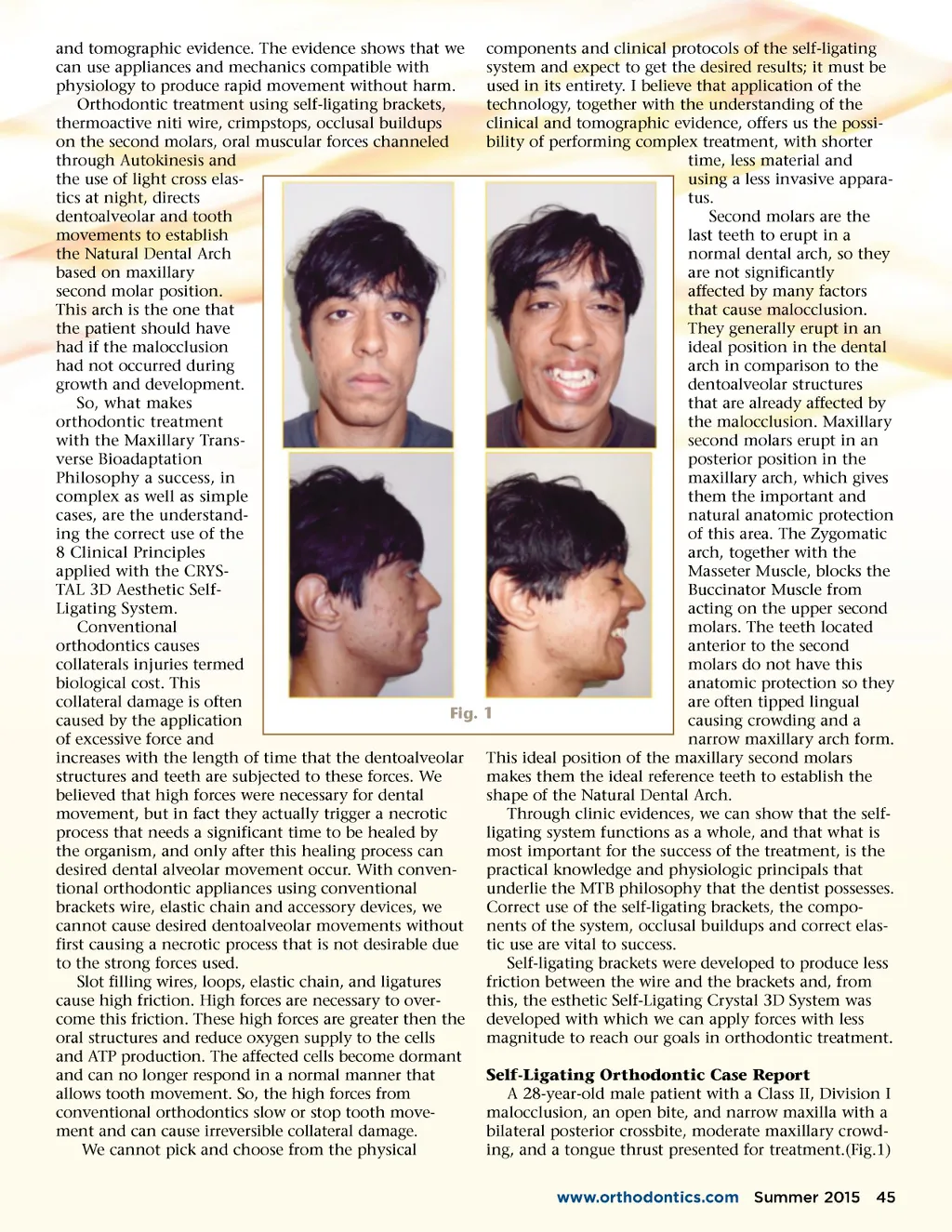
and tomographic evidence. The evidence shows that we can use appliances and mechanics compatible with physiology to produce rapid movement without harm. Orthodontic treatment using self-ligating brackets, thermoactive niti wire, crimpstops, occlusal buildups on the second molars, oral muscular forces channeled through Autokinesis and the use of light cross elas-tics at night, directs dentoalveolar and tooth movements to establish the Natural Dental Arch based on maxillary second molar position. This arch is the one that the patient should have had if the malocclusion had not occurred during growth and development. So, what makes orthodontic treatment with the Maxillary Trans-verse Bioadaptation Philosophy a success, in complex as well as simple cases, are the understand-ing the correct use of the 8 Clinical Principles applied with the CRYS-TAL 3D Aesthetic Self-Ligating System. Conventional orthodontics causes collaterals injuries termed biological cost. This collateral damage is often Fig. caused by the application of excessive force and increases with the length of time that the dentoalveolar structures and teeth are subjected to these forces. We believed that high forces were necessary for dental movement, but in fact they actually trigger a necrotic process that needs a significant time to be healed by the organism, and only after this healing process can desired dental alveolar movement occur. With conven-tional orthodontic appliances using conventional brackets wire, elastic chain and accessory devices, we cannot cause desired dentoalveolar movements without first causing a necrotic process that is not desirable due to the strong forces used. Slot filling wires, loops, elastic chain, and ligatures cause high friction. High forces are necessary to over-come this friction. These high forces are greater then the oral structures and reduce oxygen supply to the cells and ATP production. The affected cells become dormant and can no longer respond in a normal manner that allows tooth movement. So, the high forces from conventional orthodontics slow or stop tooth move-ment and can cause irreversible collateral damage. We cannot pick and choose from the physical components and clinical protocols of the self-ligating system and expect to get the desired results; it must be used in its entirety. I believe that application of the technology, together with the understanding of the clinical and tomographic evidence, offers us the possi-bility of performing complex treatment, with shorter time, less material and using a less invasive appara-tus. Second molars are the last teeth to erupt in a normal dental arch, so they are not significantly affected by many factors that cause malocclusion. They generally erupt in an ideal position in the dental arch in comparison to the dentoalveolar structures that are already affected by the malocclusion. Maxillary second molars erupt in an posterior position in the maxillary arch, which gives them the important and natural anatomic protection of this area. The Zygomatic arch, together with the Masseter Muscle, blocks the Buccinator Muscle from acting on the upper second molars. The teeth located anterior to the second molars do not have this anatomic protection so they are often tipped lingual 1 causing crowding and a narrow maxillary arch form. This ideal position of the maxillary second molars makes them the ideal reference teeth to establish the shape of the Natural Dental Arch. Through clinic evidences, we can show that the self-ligating system functions as a whole, and that what is most important for the success of the treatment, is the practical knowledge and physiologic principals that underlie the MTB philosophy that the dentist possesses. Correct use of the self-ligating brackets, the compo-nents of the system, occlusal buildups and correct elas-tic use are vital to success. Self-ligating brackets were developed to produce less friction between the wire and the brackets and, from this, the esthetic Self-Ligating Crystal 3D System was developed with which we can apply forces with less magnitude to reach our goals in orthodontic treatment. Self-Ligating Orthodontic Case Report A 28-year-old male patient with a Class II, Division I malocclusion, an open bite, and narrow maxilla with a bilateral posterior crossbite, moderate maxillary crowd-ing, and a tongue thrust presented for treatment.(Fig.1) www.orthodontics.com Summer 2015 45
Journal of the American Orthodontic Society Summer 2015-Buyer's Guide: Page 45