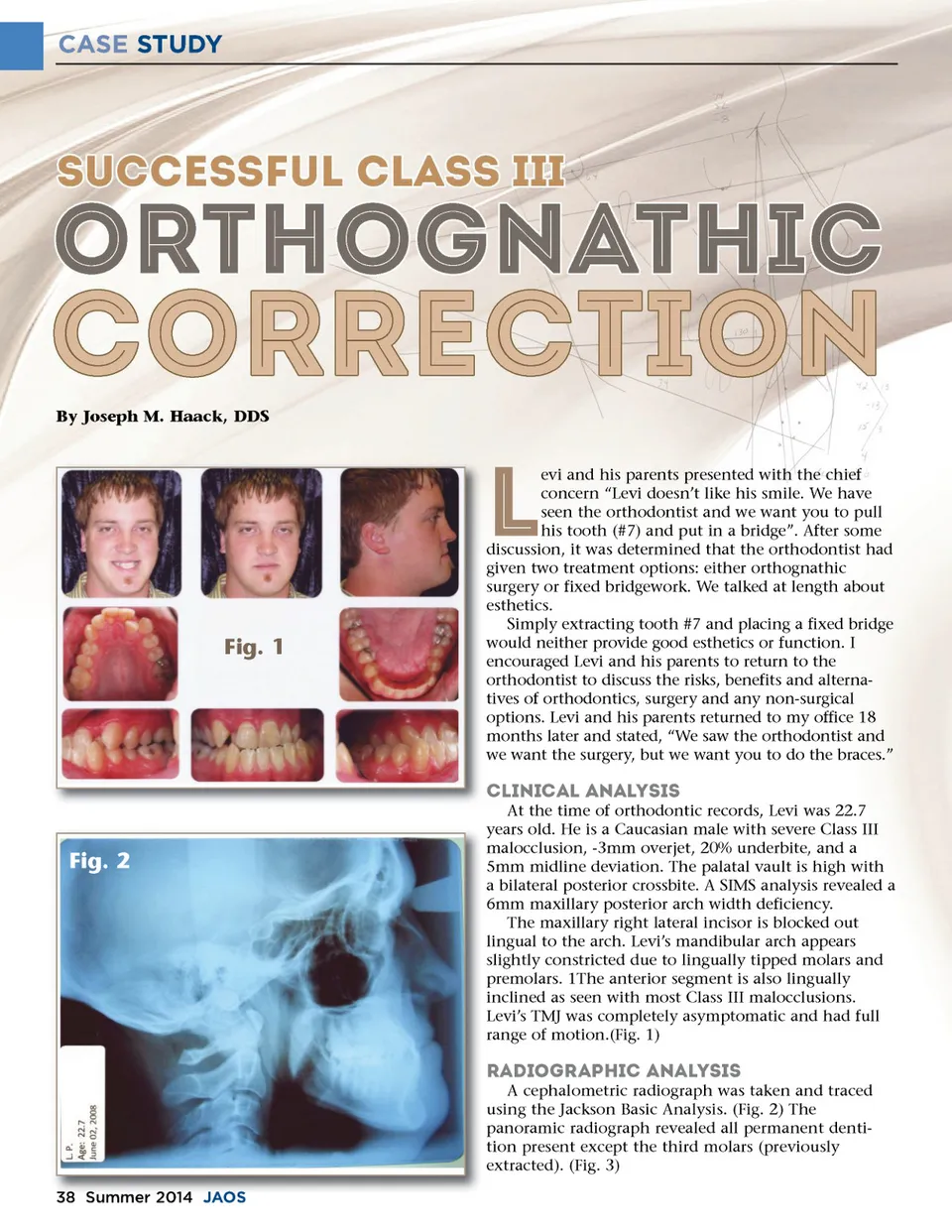
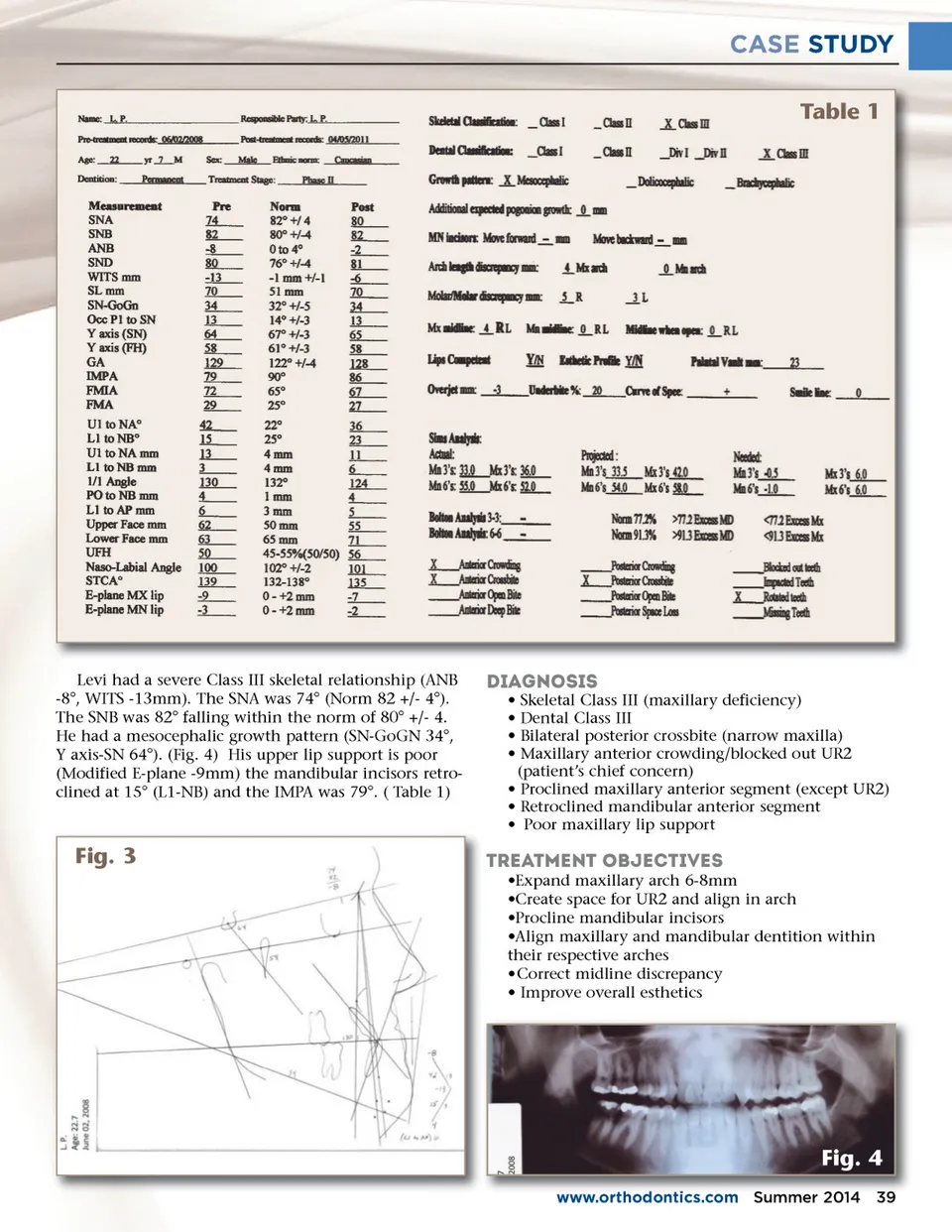
CASE STUDY By Joseph M. Haack, DDS L Fig. 1 evi and his parents presented with the chief concern “Levi doesn’t like his smile. We have seen the orthodontist and we want you to pull his tooth (#7) and put in a bridge”. After some discussion, it was determined that the orthodontist had given two treatment options: either orthognathic surgery or fixed bridgework. We talked at length about esthetics. Simply extracting tooth #7 and placing a fixed bridge would neither provide good esthetics or function. I encouraged Levi and his parents to return to the orthodontist to discuss the risks, benefits and alterna-tives of orthodontics, surgery and any non-surgical options. Levi and his parents returned to my office 18 months later and stated, “We saw the orthodontist and we want the surgery, but we want you to do the braces.” Clinical Analysis At the time of orthodontic records, Levi was 22.7 years old. He is a Caucasian male with severe Class III malocclusion, -3mm overjet, 20% underbite, and a 5mm midline deviation. The palatal vault is high with a bilateral posterior crossbite. A SIMS analysis revealed a 6mm maxillary posterior arch width deficiency. The maxillary right lateral incisor is blocked out lingual to the arch. Levi’s mandibular arch appears slightly constricted due to lingually tipped molars and premolars. 1The anterior segment is also lingually inclined as seen with most Class III malocclusions. Levi’s TMJ was completely asymptomatic and had full range of motion.(Fig. 1) Fig. 2 Radiographic Analysis A cephalometric radiograph was taken and traced using the Jackson Basic Analysis. (Fig. 2) The panoramic radiograph revealed all permanent denti-tion present except the third molars (previously extracted). (Fig. 3) 38 Summer 2014 J JAOS AOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 38