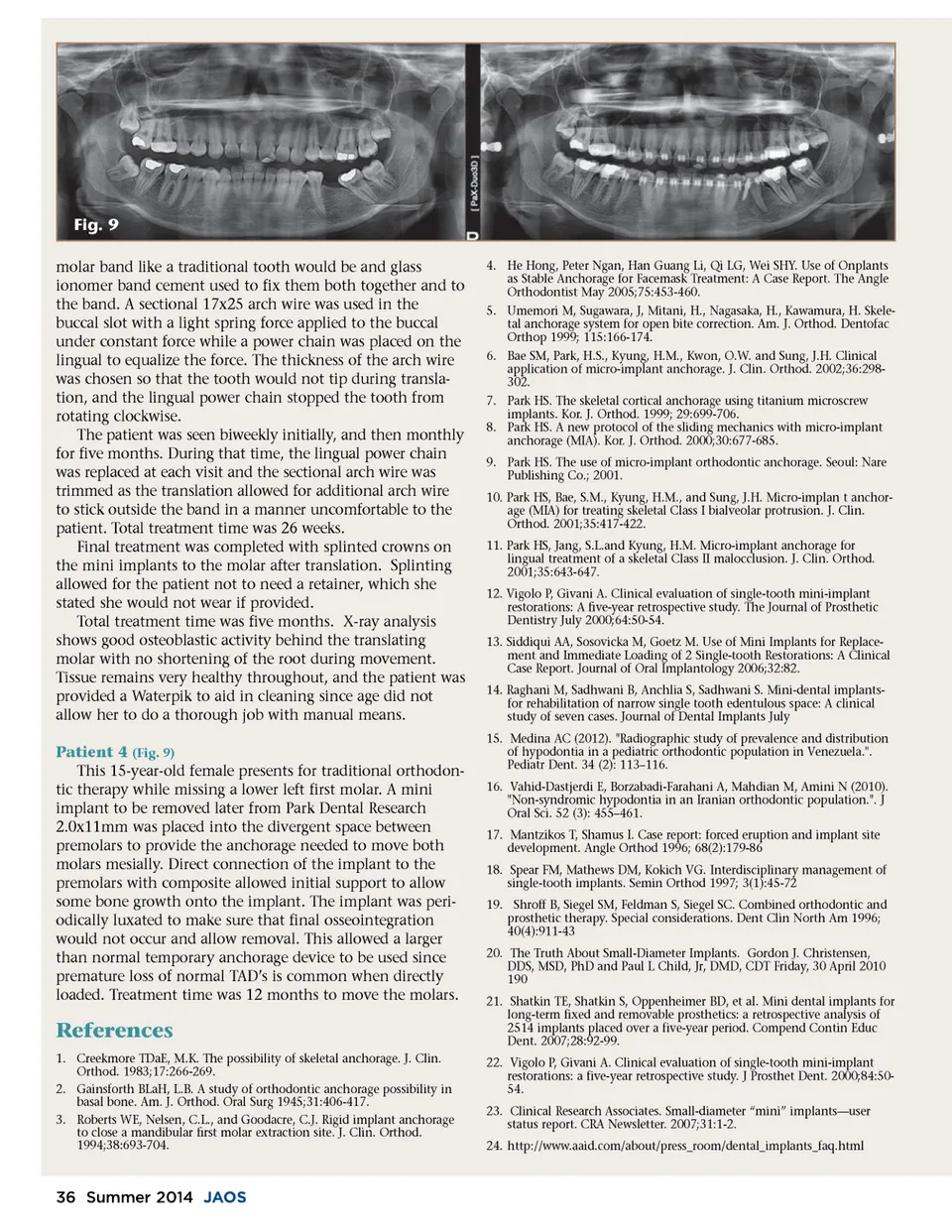
Fig. 9 molar band like a traditional tooth would be and glass ionomer band cement used to fix them both together and to the band. A sectional 17x25 arch wire was used in the buccal slot with a light spring force applied to the buccal under constant force while a power chain was placed on the lingual to equalize the force. The thickness of the arch wire was chosen so that the tooth would not tip during transla-tion, and the lingual power chain stopped the tooth from rotating clockwise. The patient was seen biweekly initially, and then monthly for five months. During that time, the lingual power chain was replaced at each visit and the sectional arch wire was trimmed as the translation allowed for additional arch wire to stick outside the band in a manner uncomfortable to the patient. Total treatment time was 26 weeks. Final treatment was completed with splinted crowns on the mini implants to the molar after translation. Splinting allowed for the patient not to need a retainer, which she stated she would not wear if provided. Total treatment time was five months. X-ray analysis shows good osteoblastic activity behind the translating molar with no shortening of the root during movement. Tissue remains very healthy throughout, and the patient was provided a Waterpik to aid in cleaning since age did not allow her to do a thorough job with manual means. Patient 4 (Fig. 9) This 15-year-old female presents for traditional orthodon-tic therapy while missing a lower left first molar. A mini implant to be removed later from Park Dental Research 2.0x11mm was placed into the divergent space between premolars to provide the anchorage needed to move both molars mesially. Direct connection of the implant to the premolars with composite allowed initial support to allow some bone growth onto the implant. The implant was peri-odically luxated to make sure that final osseointegration would not occur and allow removal. This allowed a larger than normal temporary anchorage device to be used since premature loss of normal TAD’s is common when directly loaded. Treatment time was 12 months to move the molars. 4. He Hong, Peter Ngan, Han Guang Li, Qi LG, Wei SHY. Use of Onplants as Stable Anchorage for Facemask Treatment: A Case Report. The Angle Orthodontist May 2005;75:453-460. 5. Umemori M, Sugawara, J, Mitani, H., Nagasaka, H., Kawamura, H. Skele-tal anchorage system for open bite correction. Am. J. Orthod. Dentofac Orthop 1999; 115:166-174. 6. Bae SM, Park, H.S., Kyung, H.M., Kwon, O.W. and Sung, J.H. Clinical application of micro-implant anchorage. J. Clin. Orthod. 2002;36:298-302. 7. Park HS. The skeletal cortical anchorage using titanium microscrew implants. Kor. J. Orthod. 1999; 29:699-706. 8. Park HS. A new protocol of the sliding mechanics with micro-implant anchorage (MIA). Kor. J. Orthod. 2000;30:677-685. 9. Park HS. The use of micro-implant orthodontic anchorage. Seoul: Nare Publishing Co.; 2001. 10. Park HS, Bae, S.M., Kyung, H.M., and Sung, J.H. Micro-implan t anchor-age (MIA) for treating skeletal Class I bialveolar protrusion. J. Clin. Orthod. 2001;35:417-422. 11. Park HS, Jang, S.L.and Kyung, H.M. Micro-implant anchorage for lingual treatment of a skeletal Class II malocclusion. J. Clin. Orthod. 2001;35:643-647. 12. Vigolo P, Givani A. Clinical evaluation of single-tooth mini-implant restorations: A five-year retrospective study. The Journal of Prosthetic Dentistry July 2000;64:50-54. 13. Siddiqui AA, Sosovicka M, Goetz M. Use of Mini Implants for Replace-ment and Immediate Loading of 2 Single-tooth Restorations: A Clinical Case Report. Journal of Oral Implantology 2006;32:82. 14. Raghani M, Sadhwani B, Anchlia S, Sadhwani S. Mini-dental implants-for rehabilitation of narrow single tooth edentulous space: A clinical study of seven cases. Journal of Dental Implants July 15. Medina AC (2012). "Radiographic study of prevalence and distribution of hypodontia in a pediatric orthodontic population in Venezuela.". Pediatr Dent. 34 (2): 113–116. 16. Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N (2010). "Non-syndromic hypodontia in an Iranian orthodontic population.". J Oral Sci. 52 (3): 455–461. 17. Mantzikos T, Shamus I. Case report: forced eruption and implant site development. Angle Orthod 1996; 68(2):179-86 18. Spear FM, Mathews DM, Kokich VG. Interdisciplinary management of single-tooth implants. Semin Orthod 1997; 3(1):45-72 19. Shroff B, Siegel SM, Feldman S, Siegel SC. Combined orthodontic and prosthetic therapy. Special considerations. Dent Clin North Am 1996; 40(4):911-43 20. The Truth About Small-Diameter Implants. Gordon J. Christensen, DDS, MSD, PhD and Paul L Child, Jr, DMD, CDT Friday, 30 April 2010 190 21. Shatkin TE, Shatkin S, Oppenheimer BD, et al. Mini dental implants for long-term fixed and removable prosthetics: a retrospective analysis of 2514 implants placed over a five-year period. Compend Contin Educ Dent. 2007;28:92-99. 22. Vigolo P, Givani A. Clinical evaluation of single-tooth mini-implant restorations: a five-year retrospective study. J Prosthet Dent. 2000;84:50-54. 23. Clinical Research Associates. Small-diameter “mini” implants—user status report. CRA Newsletter. 2007;31:1-2. 24. http://www.aaid.com/about/press_room/dental_implants_faq.html References 1. Creekmore TDaE, M.K. The possibility of skeletal anchorage. J. Clin. Orthod. 1983;17:266-269. 2. Gainsforth BLaH, L.B. A study of orthodontic anchorage possibility in basal bone. Am. J. Orthod. Oral Surg 1945;31:406-417. 3. Roberts WE, Nelsen, C.L., and Goodacre, C.J. Rigid implant anchorage to close a mandibular first molar extraction site. J. Clin. Orthod. 1994;38:693-704. 36 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 36