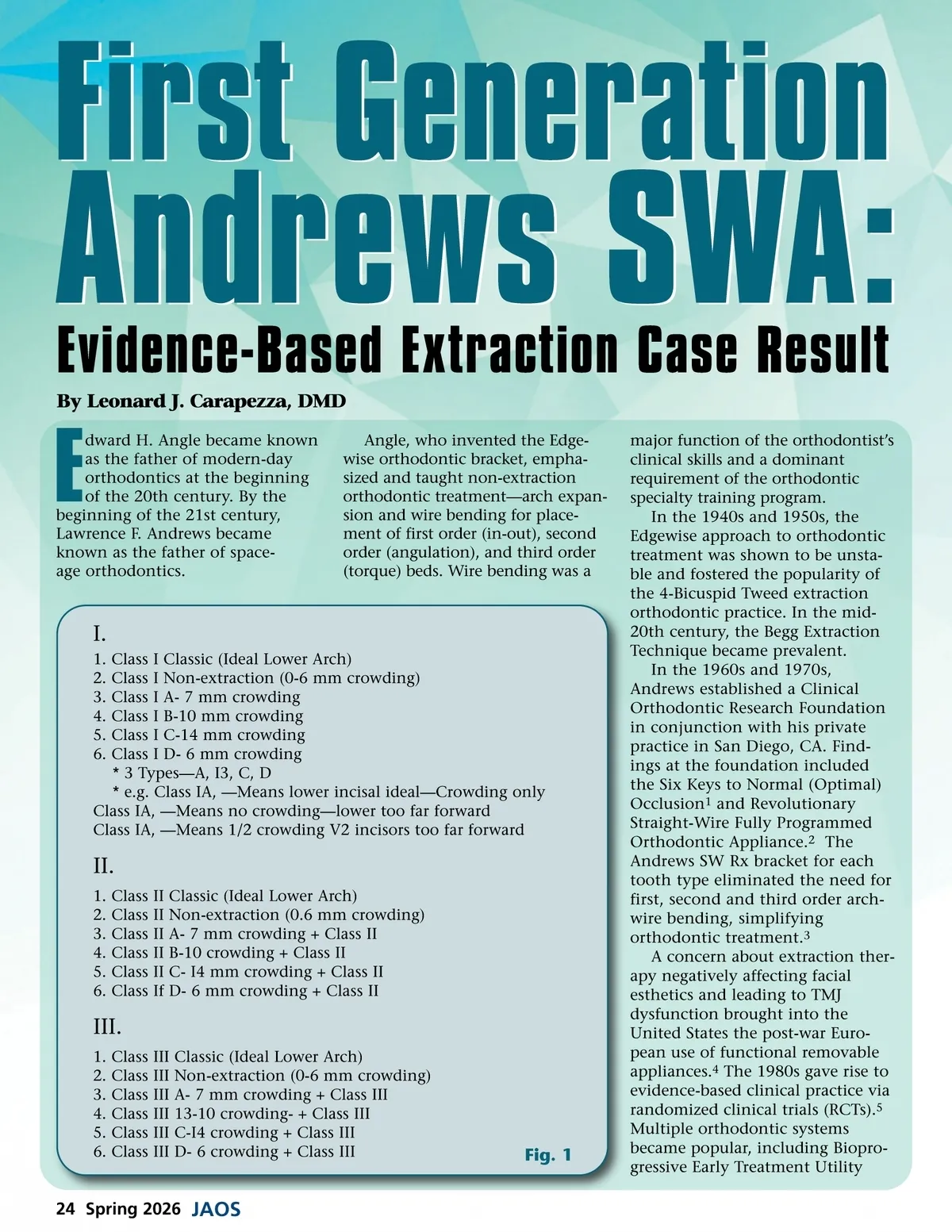
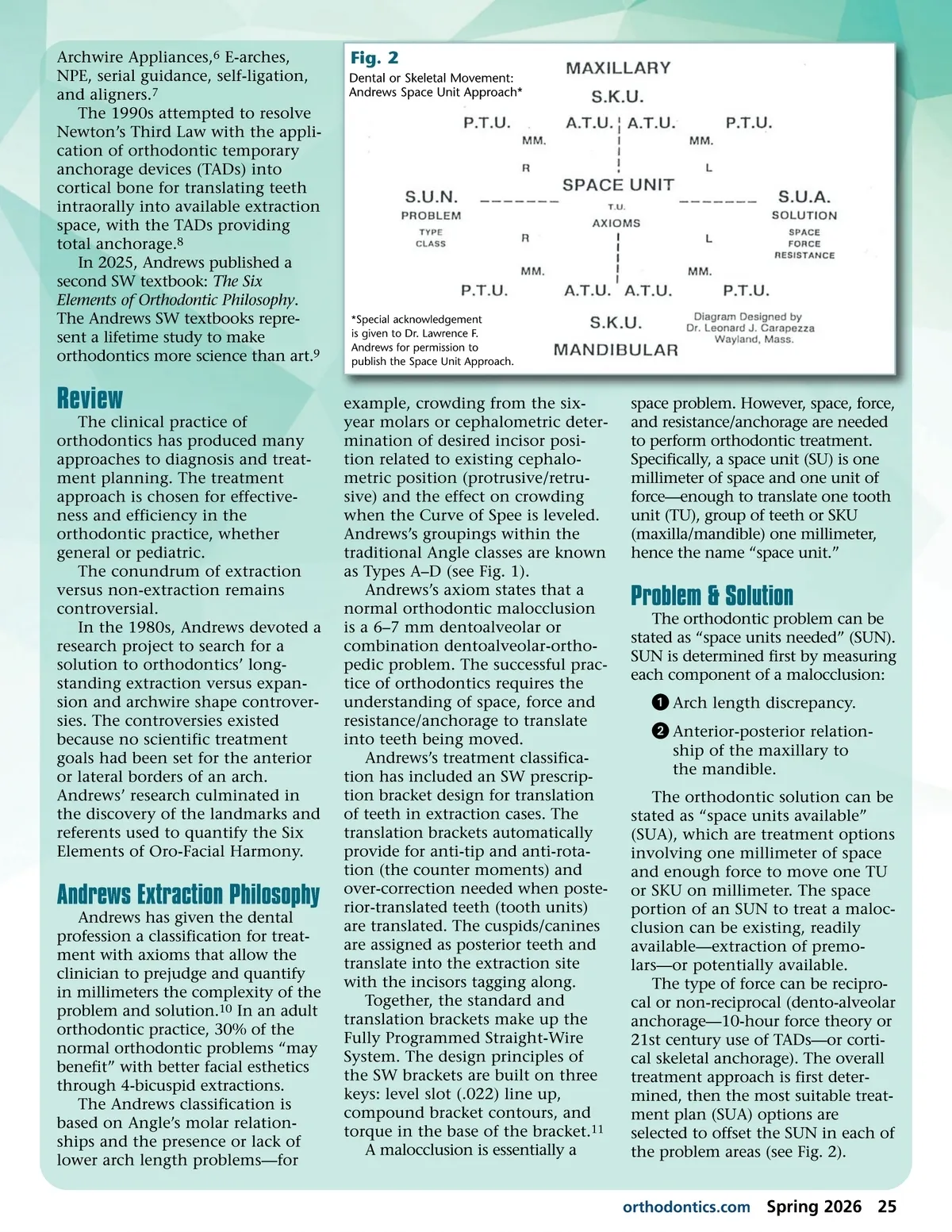
Archwire Appliances, 6 E-arches, NPE, serial guidance, self-ligation, and aligners. 7 The 1990s attempted to resolve Newton’s Third Law with the appli-cation of orthodontic temporary anchorage devices (TADs) into cortical bone for translating teeth intraorally into available extraction space, with the TADs providing total anchorage. 8 In 2025, Andrews published a second SW textbook: The Six Elements of Orthodontic Philosophy . The Andrews SW textbooks repre-sent a lifetime study to make orthodontics more science than art. 9 Fig. 2 Dental or Skeletal Movement: Andrews Space Unit Approach* *Special acknowledgement is given to Dr. Lawrence F. Andrews for permission to publish the Space Unit Approach. Review The clinical practice of orthodontics has produced many approaches to diagnosis and treat-ment planning. The treatment approach is chosen for effective-ness and efficiency in the orthodontic practice, whether general or pediatric. The conundrum of extraction versus non-extraction remains controversial. In the 1980s, Andrews devoted a research project to search for a solution to orthodontics’ long-standing extraction versus expan-sion and archwire shape controver-sies. The controversies existed because no scientific treatment goals had been set for the anterior or lateral borders of an arch. Andrews’ research culminated in the discovery of the landmarks and referents used to quantify the Six Elements of Oro-Facial Harmony. Andrews Extraction Philosophy Andrews has given the dental profession a classification for treat-ment with axioms that allow the clinician to prejudge and quantify in millimeters the complexity of the problem and solution. 10 In an adult orthodontic practice, 30% of the normal orthodontic problems “may benefit” with better facial esthetics through 4-bicuspid extractions. The Andrews classification is based on Angle’s molar relation-ships and the presence or lack of lower arch length problems—for example, crowding from the six-year molars or cephalometric deter-mination of desired incisor posi-tion related to existing cephalo-metric position (protrusive/retru-sive) and the effect on crowding when the Curve of Spee is leveled. Andrews’s groupings within the traditional Angle classes are known as Types A–D (see Fig. 1). Andrews’s axiom states that a normal orthodontic malocclusion is a 6–7 mm dentoalveolar or combination dentoalveolar-ortho-pedic problem. The successful prac-tice of orthodontics requires the understanding of space, force and resistance/anchorage to translate into teeth being moved. Andrews’s treatment classifica-tion has included an SW prescrip-tion bracket design for translation of teeth in extraction cases. The translation brackets automatically provide for anti-tip and anti-rota-tion (the counter moments) and over-correction needed when poste-rior-translated teeth (tooth units) are translated. The cuspids/canines are assigned as posterior teeth and translate into the extraction site with the incisors tagging along. Together, the standard and translation brackets make up the Fully Programmed Straight-Wire System. The design principles of the SW brackets are built on three keys: level slot (.022) line up, compound bracket contours, and torque in the base of the bracket. 11 A malocclusion is essentially a space problem. However, space, force, and resistance/anchorage are needed to perform orthodontic treatment. Specifically, a space unit (SU) is one millimeter of space and one unit of force—enough to translate one tooth unit (TU), group of teeth or SKU (maxilla/mandible) one millimeter, hence the name “space unit.” Problem & Solution The orthodontic problem can be stated as “space units needed” (SUN). SUN is determined first by measuring each component of a malocclusion: ᕡ Arch length discrepancy. ᕢ Anterior-posterior relation-ship of the maxillary to the mandible. The orthodontic solution can be stated as “space units available” (SUA), which are treatment options involving one millimeter of space and enough force to move one TU or SKU on millimeter. The space portion of an SUN to treat a maloc-clusion can be existing, readily available—extraction of premo-lars—or potentially available. The type of force can be recipro-cal or non-reciprocal (dento-alveolar anchorage—10-hour force theory or 21st century use of TADs—or corti-cal skeletal anchorage). The overall treatment approach is first deter-mined, then the most suitable treat-ment plan (SUA) options are selected to offset the SUN in each of the problem areas (see Fig. 2). orthodontics.com Spring 2026 25
Journal of the American Orthodontic Society Spring 2026: Page 25