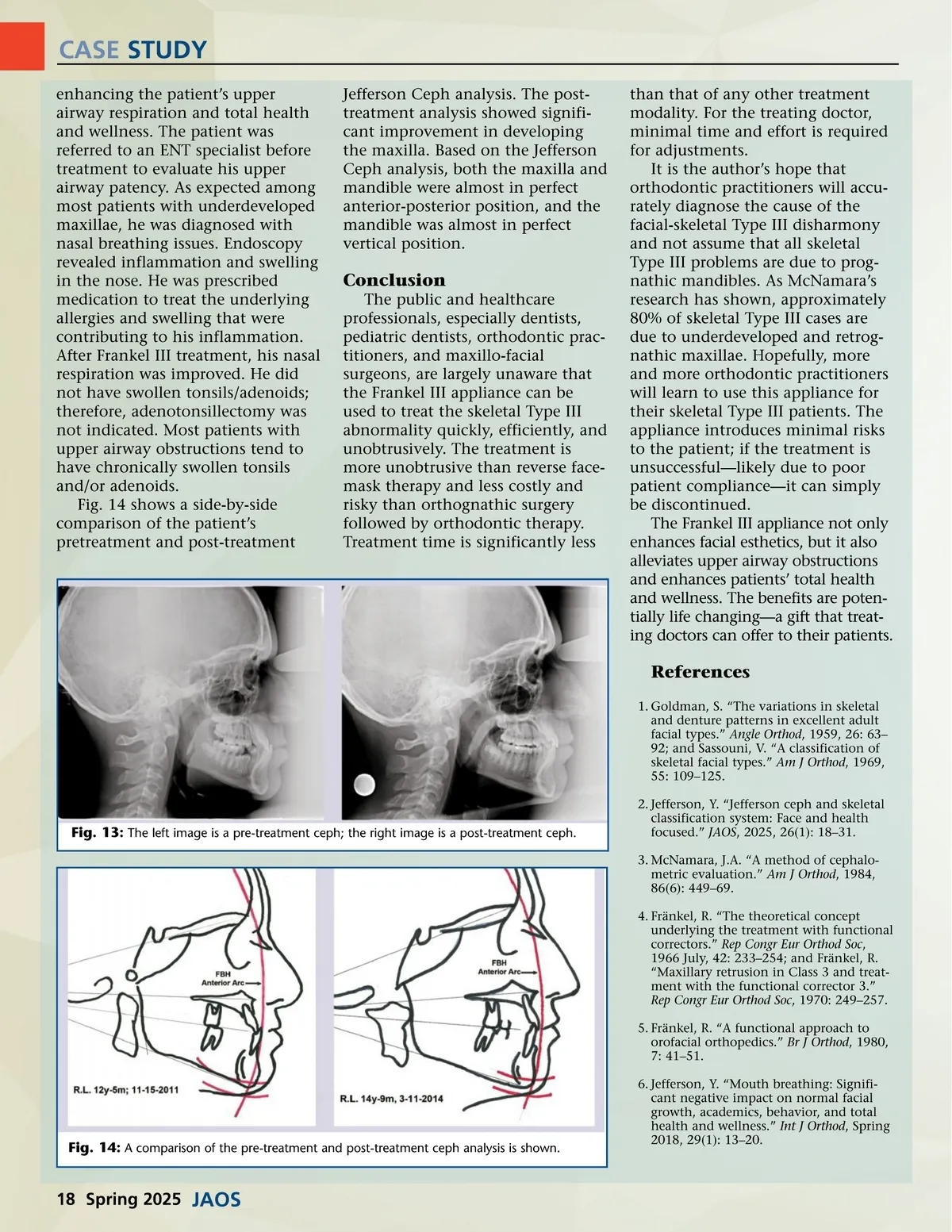
CASE STUDY enhancing the patient’s upper airway respiration and total health and wellness. The patient was referred to an ENT specialist before treatment to evaluate his upper airway patency. As expected among most patients with underdeveloped maxillae, he was diagnosed with nasal breathing issues. Endoscopy revealed inflammation and swelling in the nose. He was prescribed medication to treat the underlying allergies and swelling that were contributing to his inflammation. After Frankel III treatment, his nasal respiration was improved. He did not have swollen tonsils/adenoids; therefore, adenotonsillectomy was not indicated. Most patients with upper airway obstructions tend to have chronically swollen tonsils and/or adenoids. Fig. 14 shows a side-by-side comparison of the patient’s pretreatment and post-treatment Jefferson Ceph analysis. The post-treatment analysis showed signifi-cant improvement in developing the maxilla. Based on the Jefferson Ceph analysis, both the maxilla and mandible were almost in perfect anterior-posterior position, and the mandible was almost in perfect vertical position. than that of any other treatment modality. For the treating doctor, minimal time and effort is required for adjustments. It is the author’s hope that orthodontic practitioners will accu-rately diagnose the cause of the facial-skeletal Type III disharmony and not assume that all skeletal Type III problems are due to prog-nathic mandibles. As McNamara’s research has shown, approximately 80% of skeletal Type III cases are due to underdeveloped and retrog-nathic maxillae. Hopefully, more and more orthodontic practitioners will learn to use this appliance for their skeletal Type III patients. The appliance introduces minimal risks to the patient; if the treatment is unsuccessful—likely due to poor patient compliance—it can simply be discontinued. The Frankel III appliance not only enhances facial esthetics, but it also alleviates upper airway obstructions and enhances patients’ total health and wellness. The benefits are poten-tially life changing—a gift that treat-ing doctors can offer to their patients. Conclusion The public and healthcare professionals, especially dentists, pediatric dentists, orthodontic prac-titioners, and maxillo-facial surgeons, are largely unaware that the Frankel III appliance can be used to treat the skeletal Type III abnormality quickly, efficiently, and unobtrusively. The treatment is more unobtrusive than reverse face-mask therapy and less costly and risky than orthognathic surgery followed by orthodontic therapy. Treatment time is significantly less References 1. Goldman, S. “The variations in skeletal and denture patterns in excellent adult facial types.” Angle Orthod , 1959, 26: 63– 92; and Sassouni, V. “A classification of skeletal facial types.” Am J Orthod , 1969, 55: 109–125. 2. Jefferson, Y. “Jefferson ceph and skeletal classification system: Face and health focused.” JAOS , 2025, 26(1): 18–31. 3. McNamara, J.A. “A method of cephalo-metric evaluation.” Am J Orthod , 1984, 86(6): 449–69. 4. Fränkel, R. “The theoretical concept underlying the treatment with functional correctors.” Rep Congr Eur Orthod Soc , 1966 July, 42: 233–254; and Fränkel, R. “Maxillary retrusion in Class 3 and treat-ment with the functional corrector 3.” Rep Congr Eur Orthod Soc , 1970: 249–257. 5. Fränkel, R. “A functional approach to orofacial orthopedics.” Br J Orthod , 1980, 7: 41–51. 6. Jefferson, Y. “Mouth breathing: Signifi-cant negative impact on normal facial growth, academics, behavior, and total health and wellness.” Int J Orthod , Spring 2018, 29(1): 13–20. Fig. 13: The left image is a pre-treatment ceph; the right image is a post-treatment ceph. Fig. 14: A comparison of the pre-treatment and post-treatment ceph analysis is shown. 18 Spring 2025 JAOS
Journal of the American Orthodontic Society Spring 2025: Page 18