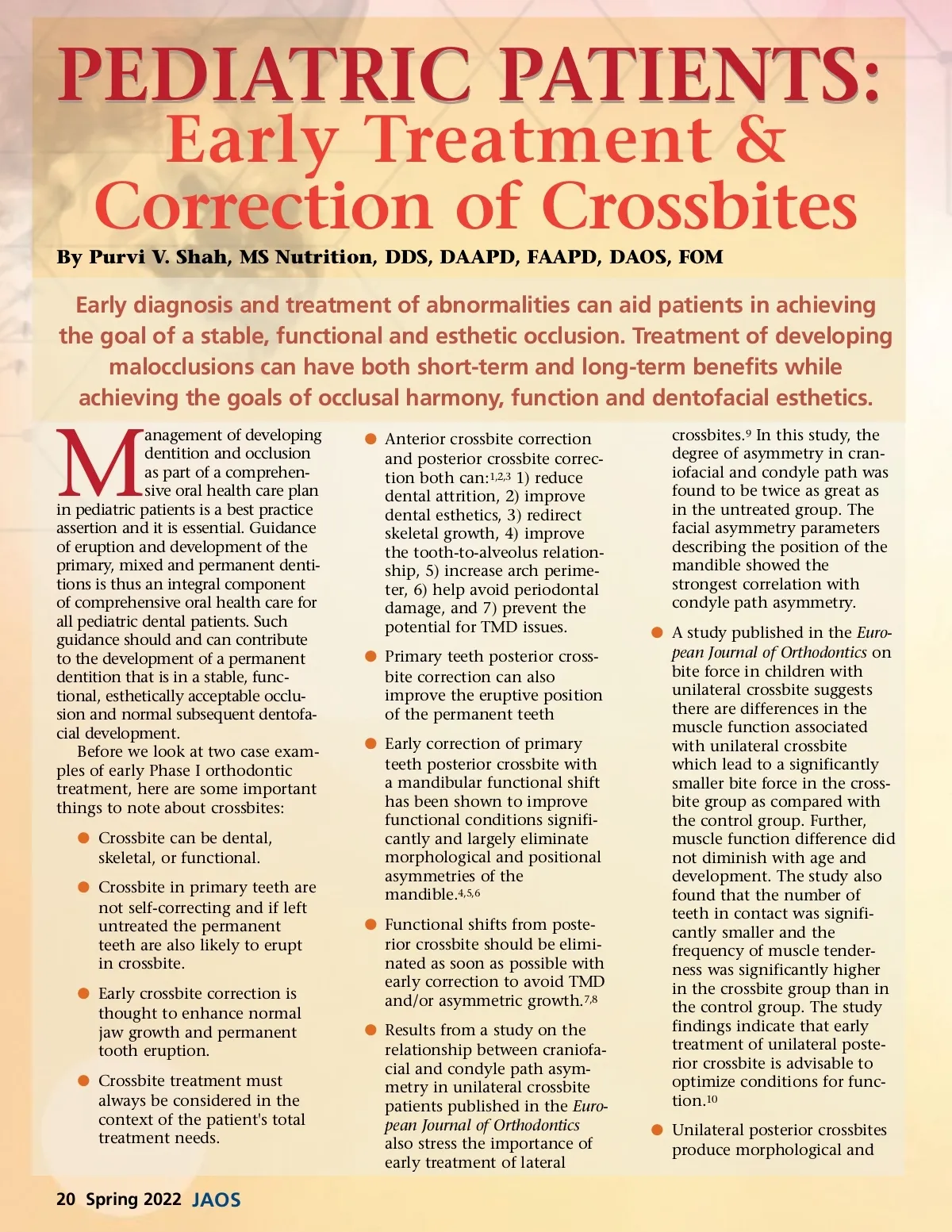
positional asymmetries of the mandible in young children. These asymmetries can largely be eliminated with early expansion therapy. 11 Skeletal expansion with fixed or removable palatal expanders can be utilized until mid-line suture fusion occurs. 12,13 b Treatment can be completed with a combination of treat-ment modalities to correct the alveolar constriction and tooth position. 14 b Crossbite treatment decisions will depend on the following considerations: • Amount and type of move-ment (tipping versus bodily movement, rotation, or dental versus orthopedic movement). • Space available. • AP, transverse, and vertical skeletal relationships. • Growth status of the child • Patient cooperation. Fig. 1 Case Examples, Phase 1 Only The following case examples will demonstrate and provide evidence and support for early diagnosis and early treatment of malocclusion, craniofacial anomalies and related conditions. In the first case, the treatment commenced at 7 years, 1 month. Patient I is a Caucasian male having a fraternal twin. The mother was concerned about the developing facial asymmetry. The mother shared that Patient I, in sharing the womb with his sister, had his right side of the face pressed against the inner wall of the uterine sac. Asym-metrical development of the right side facial muscles of the patient deviates to the left is noticeable when he opens his mouth. This as explained to the mother by her obstetrician and child’s pediatrician could have been caused by the patient’s positional placement. On analysis of the case, it was explained to the mother that the skeletal and dental crossbite was due to the facial muscle asymmetry and she was advised about the impact it would have on the child’s future craniofacial dental develop-ment. The mother was seeking limited treatment to correct the anterior and posterior crossbite. The patient’s medical history included swollen tonsils and Esthetic Occlusion Correct and appropriate orthodon-tic treatment, performed at the right time, can not only create a beautiful smile and a functionally better and esthetic occlusion, but can also help prevent and/or cure tooth pain in children caused by severe malocclu-sion. It can reduce dental attrition and wear on primary and permanent teeth and can help children gain (or regain) self-confidence from improved dental esthetics. Children experiencing teasing or bullying due to their compro-mised dental esthetics from a crossbite can also avail social and psychological benefits of an improved smile achieved from undergoing crossbite treatment. Further, the right intervention and orthodontic treatment in chil-dren still in their development stage of life can: b Redirect and help improve skeletal growth b Improve the tooth-to-alveolus relationship b Increase arch perimeter b Help avoid periodontal damage to the lower incisors, and b Prevent the potential for TMD issues adenoids, disrupted sleep pattern and teeth grinding at night. Patient I’s dental examination showed: b Mixed dentition b Pain on chewing with anterior teeth in crossbite b High appearing narrow palate vault b Anterior and posterior crossbite b Dental midline is on b Asymmetric smile b Deep-bite -locked occlu-sion/mandible b Anterior mnimal overjet b Class II malocclusion b Short turned up maxillary lip b A one-half Class II molar rela-tionship, a 90% overbite b When the muscles of facial expression are evaluated, there appeared to be intermittent weakness of his right marginal mandibular branch. However, this was difficult to reproduce and did not appear to be present during all movements b Mesocephalic and a straight profile. (Fig. 1) www.orthodontics.com Spring 2022 21
Journal of the American Orthodontic Society Spring 2022: Page 21