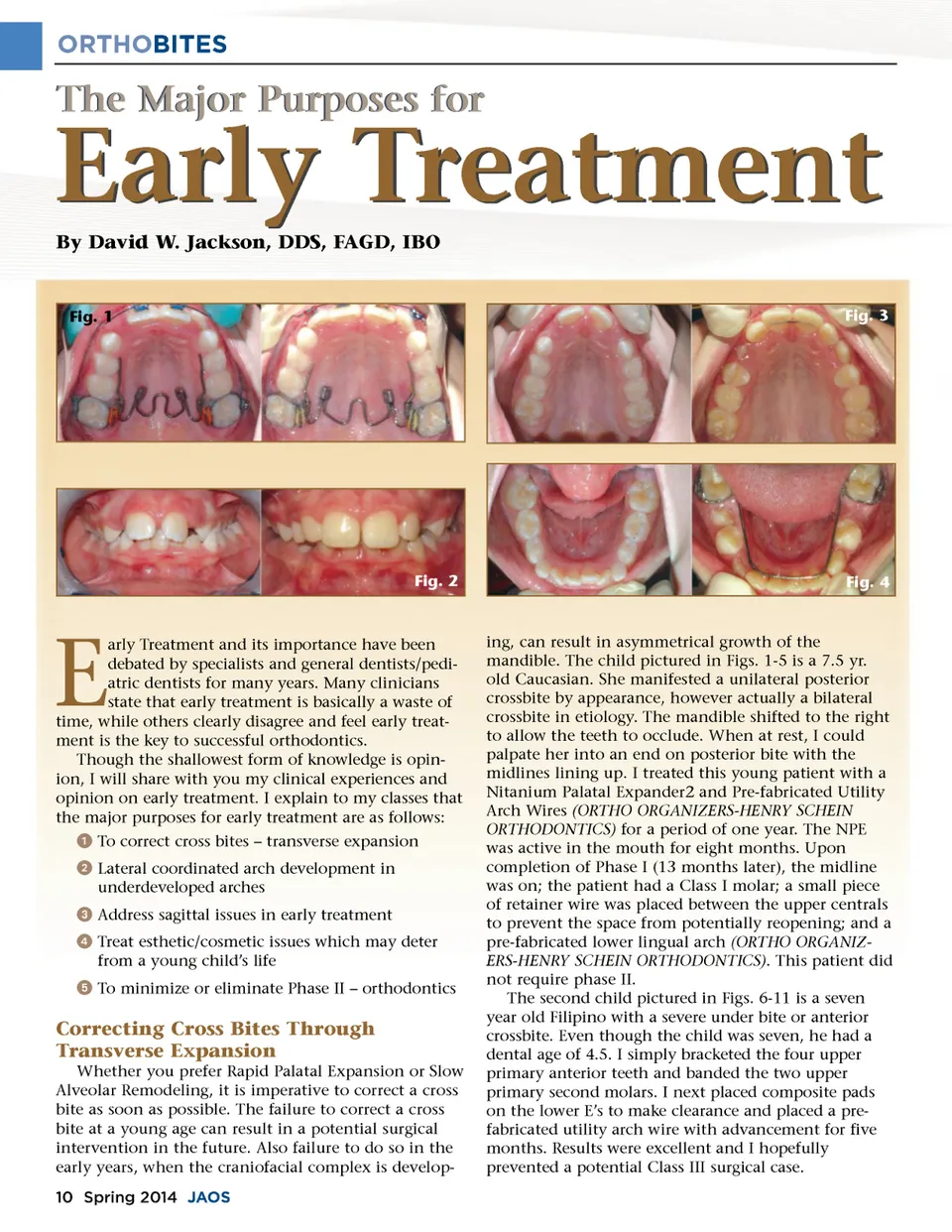
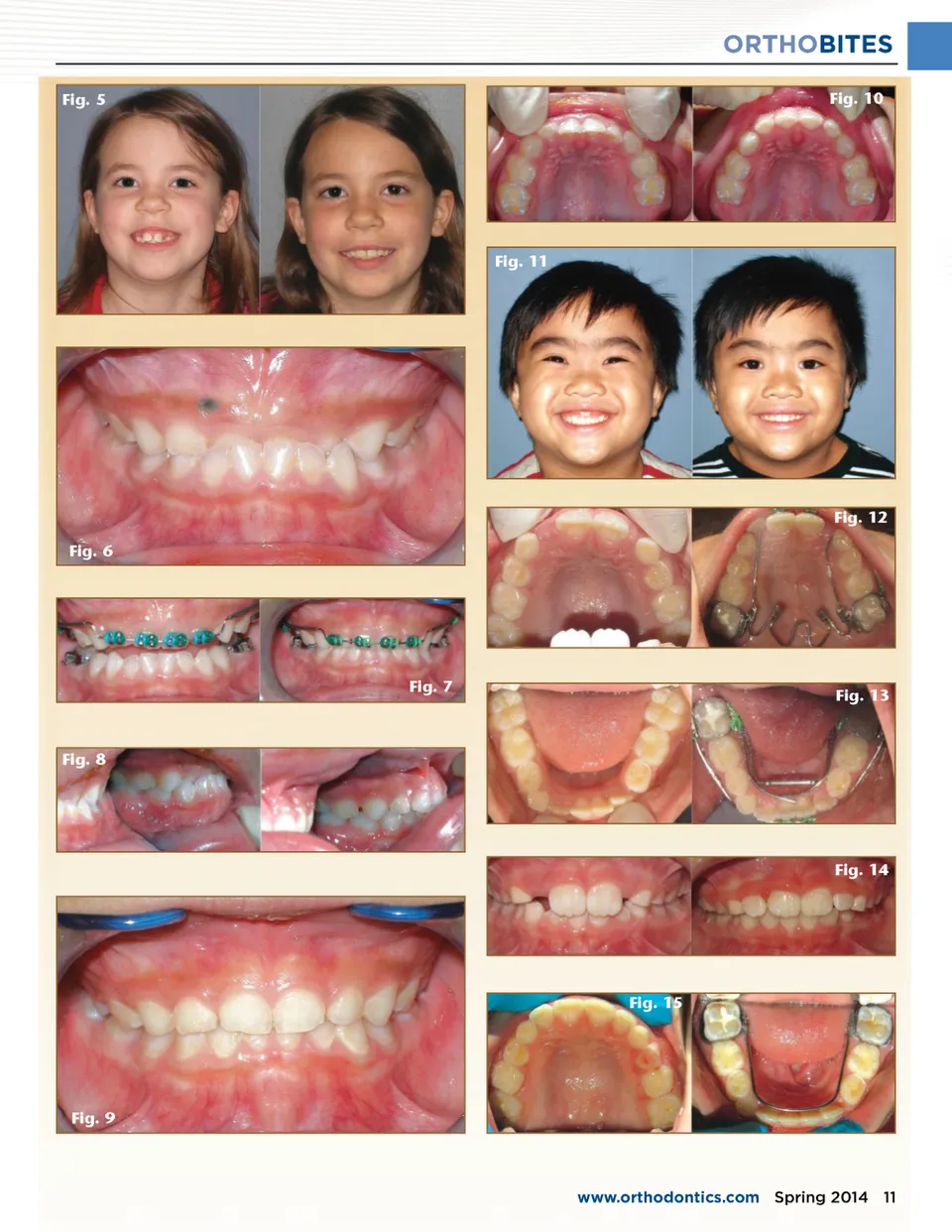
ORTHOBITES The Major Purposes for Early Treatment By David W. Jackson, DDS, FAGD, IBO Fig. 1 Fig. 3 Fig. 2 Fig. 4 E arly Treatment and its importance have been debated by specialists and general dentists/pedi-atric dentists for many years. Many clinicians state that early treatment is basically a waste of time, while others clearly disagree and feel early treat-ment is the key to successful orthodontics. Though the shallowest form of knowledge is opin-ion, I will share with you my clinical experiences and opinion on early treatment. I explain to my classes that the major purposes for early treatment are as follows: ᕡ To correct cross bites – transverse expansion ᕢ Lateral coordinated arch development in underdeveloped arches ᕣ Address sagittal issues in early treatment ᕤ Treat esthetic/cosmetic issues which may deter from a young child’s life ᕥ To minimize or eliminate Phase II – orthodontics Correcting Cross Bites Through Transverse Expansion Whether you prefer Rapid Palatal Expansion or Slow Alveolar Remodeling, it is imperative to correct a cross bite as soon as possible. The failure to correct a cross bite at a young age can result in a potential surgical intervention in the future. Also failure to do so in the early years, when the craniofacial complex is develop-10 Spring 2014 JAOS ing, can result in asymmetrical growth of the mandible. The child pictured in Figs. 1-5 is a 7.5 yr. old Caucasian. She manifested a unilateral posterior crossbite by appearance, however actually a bilateral crossbite in etiology. The mandible shifted to the right to allow the teeth to occlude. When at rest, I could palpate her into an end on posterior bite with the midlines lining up. I treated this young patient with a Nitanium Palatal Expander2 and Pre-fabricated Utility Arch Wires (ORTHO ORGANIZERS-HENRY SCHEIN ORTHODONTICS) for a period of one year. The NPE was active in the mouth for eight months. Upon completion of Phase I (13 months later), the midline was on; the patient had a Class I molar; a small piece of retainer wire was placed between the upper centrals to prevent the space from potentially reopening; and a pre-fabricated lower lingual arch (ORTHO ORGANIZ-ERS-HENRY SCHEIN ORTHODONTICS) . This patient did not require phase II. The second child pictured in Figs. 6-11 is a seven year old Filipino with a severe under bite or anterior crossbite. Even though the child was seven, he had a dental age of 4.5. I simply bracketed the four upper primary anterior teeth and banded the two upper primary second molars. I next placed composite pads on the lower E’s to make clearance and placed a pre-fabricated utility arch wire with advancement for five months. Results were excellent and I hopefully prevented a potential Class III surgical case.
Journal of the American Orthodontic Society Spring 2014: Page 10