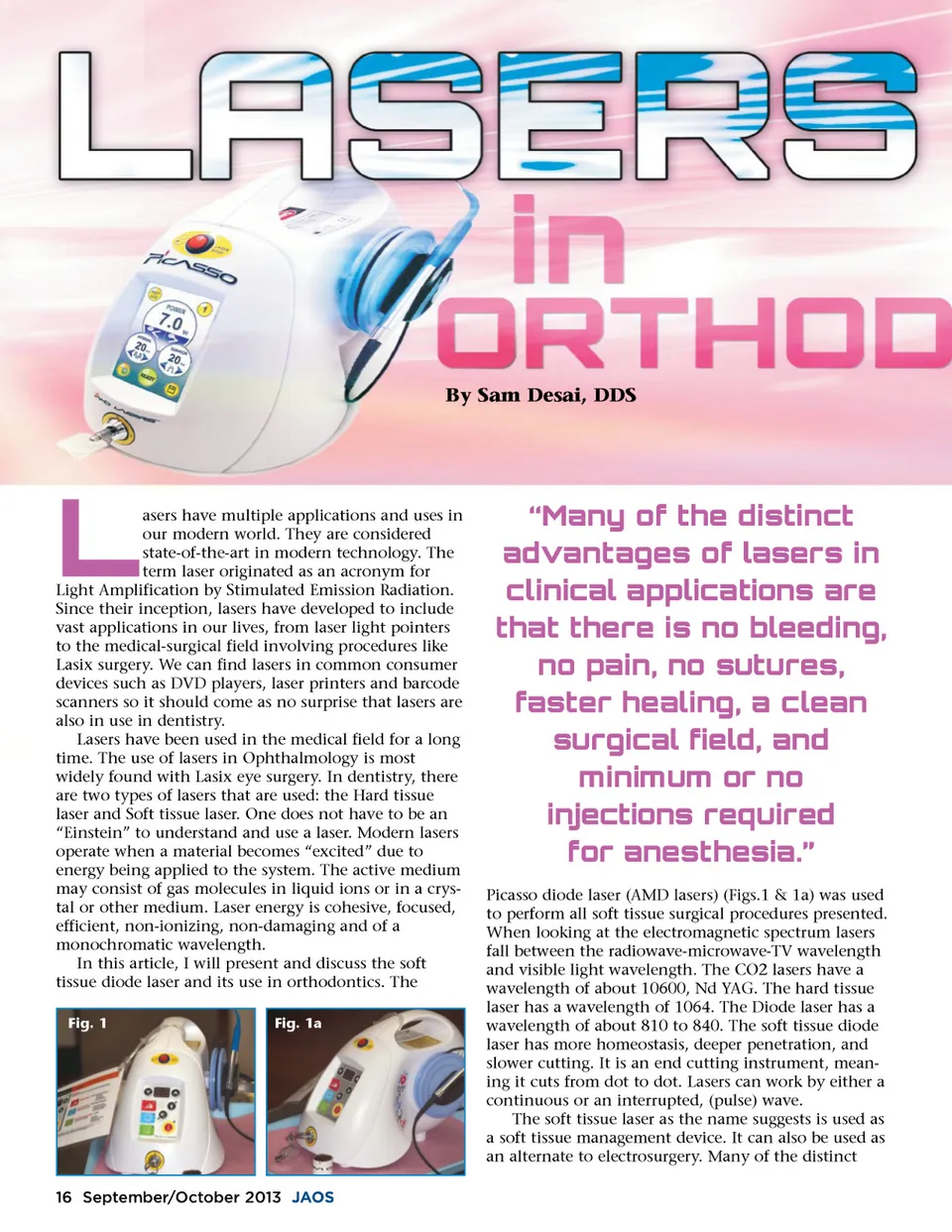
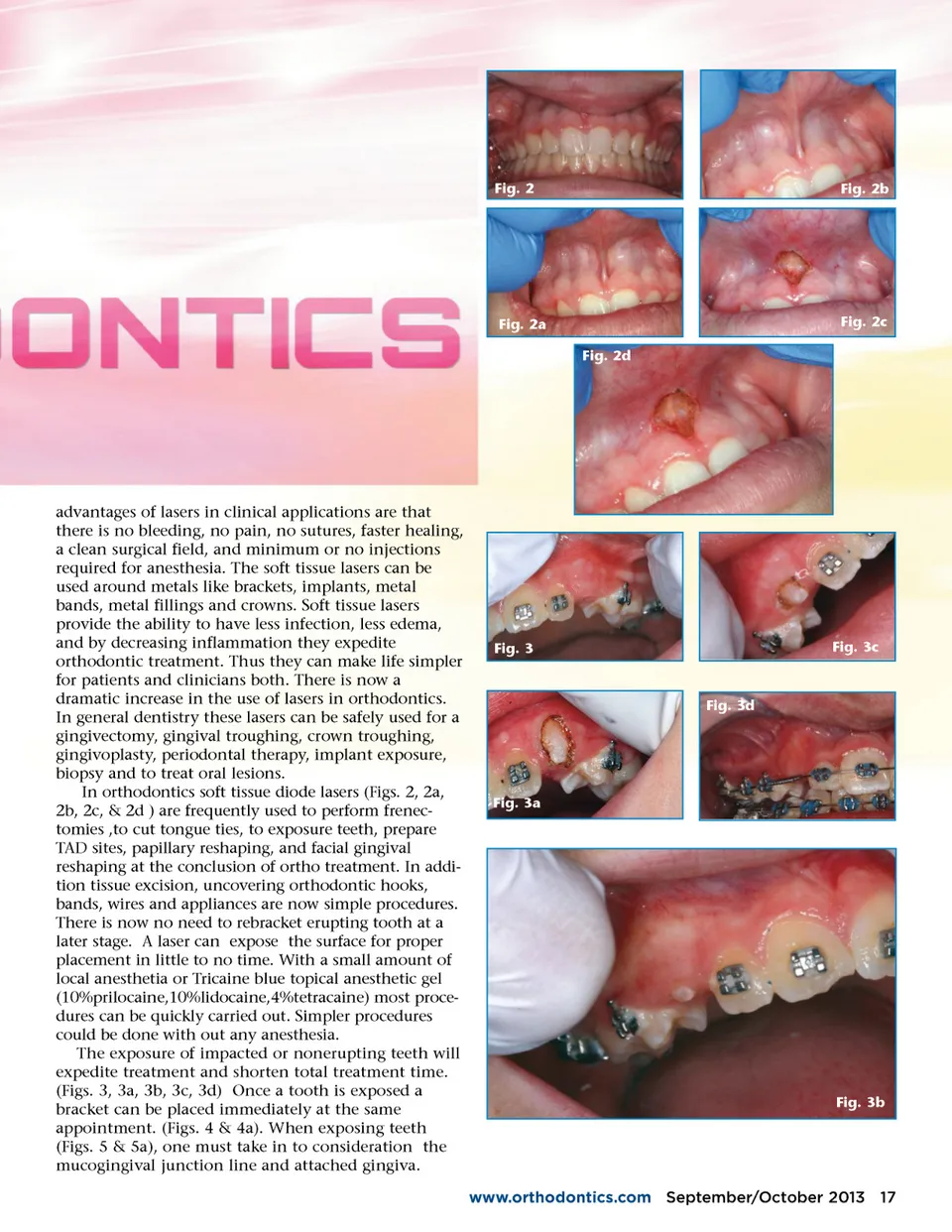
Fig. 2 Fig. 2b Fig. 2a Fig. 2d Fig. 2c advantages of lasers in clinical applications are that there is no bleeding, no pain, no sutures, faster healing, a clean surgical field, and minimum or no injections required for anesthesia. The soft tissue lasers can be used around metals like brackets, implants, metal bands, metal fillings and crowns. Soft tissue lasers provide the ability to have less infection, less edema, and by decreasing inflammation they expedite orthodontic treatment. Thus they can make life simpler for patients and clinicians both. There is now a dramatic increase in the use of lasers in orthodontics. In general dentistry these lasers can be safely used for a gingivectomy, gingival troughing, crown troughing, gingivoplasty, periodontal therapy, implant exposure, biopsy and to treat oral lesions. In orthodontics soft tissue diode lasers (Figs. 2, 2a, 2b, 2c, & 2d ) are frequently used to perform frenec-tomies ,to cut tongue ties, to exposure teeth, prepare TAD sites, papillary reshaping, and facial gingival reshaping at the conclusion of ortho treatment. In addi-tion tissue excision, uncovering orthodontic hooks, bands, wires and appliances are now simple procedures. There is now no need to rebracket erupting tooth at a later stage. A laser can expose the surface for proper placement in little to no time. With a small amount of local anesthetia or Tricaine blue topical anesthetic gel (10%prilocaine,10%lidocaine,4%tetracaine) most proce-dures can be quickly carried out. Simpler procedures could be done with out any anesthesia. The exposure of impacted or nonerupting teeth will expedite treatment and shorten total treatment time. (Figs. 3, 3a, 3b, 3c, 3d) Once a tooth is exposed a bracket can be placed immediately at the same appointment. (Figs. 4 & 4a). When exposing teeth (Figs. 5 & 5a), one must take in to consideration the mucogingival junction line and attached gingiva. Fig. 3 Fig. 3c Fig. 3d Fig. 3a Fig. 3b www.orthodontics.com September/October 2013 17
Journal of the American Orthodontic Society September-October 2013: Page 17