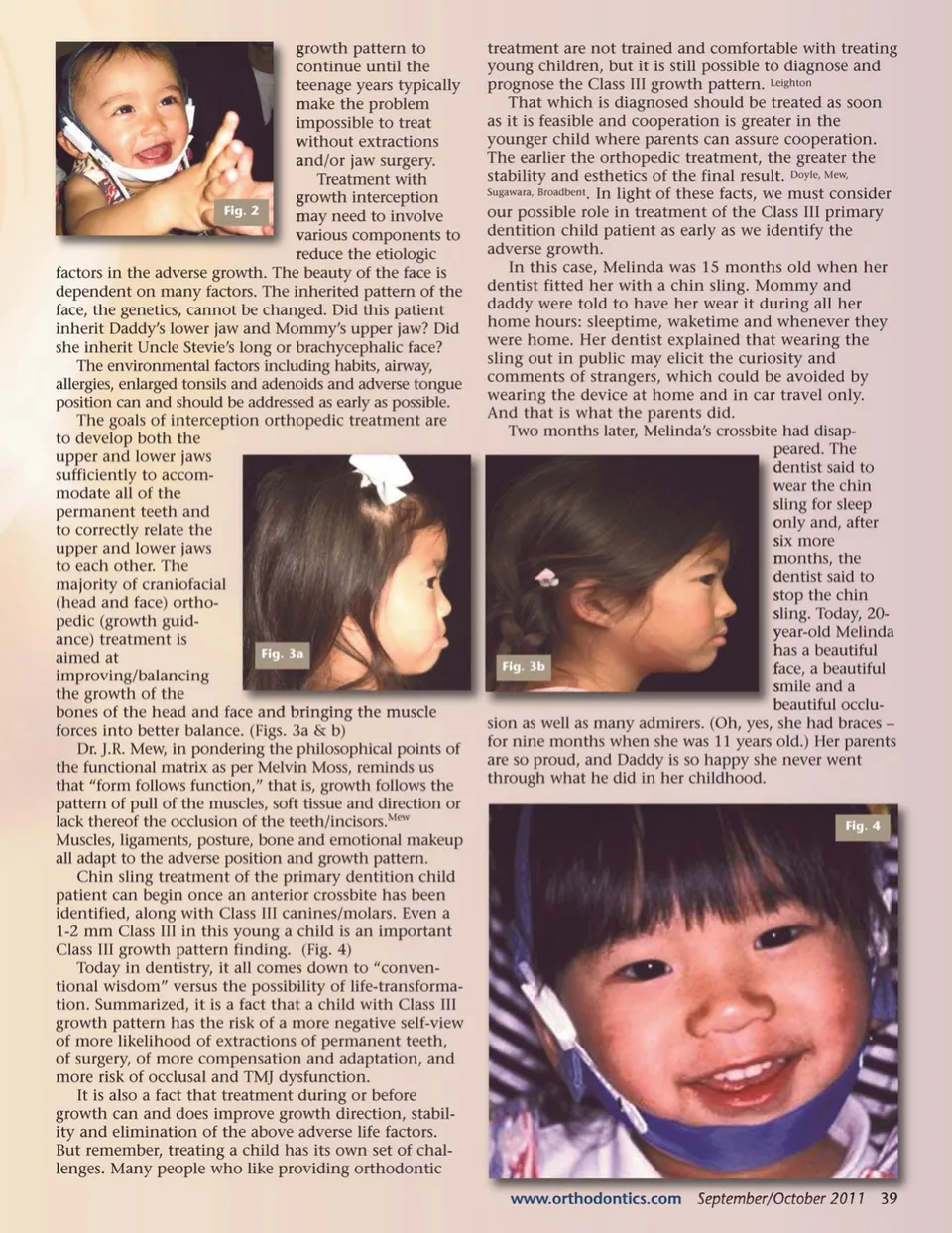
GOALS of INTERCEPTION i ORTHODONTIC TREATMENT By Chris Baker, RN, DMD Melinda is such a sweet baby. Her mommy and daddy are so proud to show her off, except that her daddy has noticed Melinda has an awfully strong jawline for a baby. He has a strong jawline, even after surgery at age 23. He doesn’t want Melinda to go through what he went through as a child: teasing from other children, and taunting from teachers and coaches who thought he was a bully. After three visits to dentists and orthodontists, Melinda and her parents have been told to wait until she has finished growing and see what her bite looks like. Her daddy is determined to find another answer. And he does; he finds a dentist who agrees that Melinda should be treated before the adverse growth has been allowed to create the need for surgery and an unattractive face throughout childhood. This dentist recommends the chin sling now. Mommy and Daddy are very happy. n underbite, or anterior crossbite, is a condition in which the lower teeth are positioned in front of the upper teeth and often a sign of a Class III growth pattern. Even if there is not a Class III growth pattern, there may be one in the near future, due to the mandibu-lar growth being uninhibited by the normal overbite and overjet of the maxillary incisors, and the maxillary growth may be inhibited by the crossbite position of the mandibular incisors. So, in effect, the growing child with a crossbite is “wearing” an appliance (the teeth in anterior crossbite), which will encourage Class III growth. And, when the incisor occlusion is reversed, which it is in a crossbite, efficient biting and chewing are impos-sible and the facial appearance is thrown off balance and is not as esthetically pleasing. (Figs. 1a & b) Traditionally in the United States, Class III treatment has been postponed until the patient has all permanent teeth, often until the patient is finished growing. All-too-often treatment options have been narrowed to a surgical solution because growth has rendered an orthopedic problem (growth of bones) unchangeable with orthodontics (movement of teeth). This thinking is based on the fact that the adverse growth causes and worsens the occlusion and the facial esthetics. However, it overlooks the probability of redirecting this adverse growth when treated in primary dentition! While adult faces exhibit various levels of beauty, all babies and little children are beautiful. The oddest little face is still gorgeous. However, being a gorgeous baby 38 September/October 2011 JAOS A Fig. 1a Fig. 1b does not guarantee a beautiful adult face. The growing toddler quickly loses the baby-face and the early rapid growth of the craniofacial structures exhibits the strong profile early and clearly on the young child’s face. The young Class III-growing child finds his/her spirit trapped with a face like Melinda’s daddy’s face, that is “tough” (people would say, “like a bull-dog”) and a face that is unattractive. This leads teachers, coaches, relatives, friends and classmates to assume the child’s personality will be “tough” (“bull-dog”) or not as sweet and not as delicate and childlike as the young child really is. And, worst of all, the child’s self-view becomes what the child’s close circle is communicating to that child. Clifford, Magli As Dr. David Satcher, U.S. Surgeon General, said in 2000, “The importance of the face as the bearer of iden-tity, character, intelligence and beauty is universal. Faces judged ugly or disharmonious, or those scarred by birth defects or injury, have been associated with defects in character, intelligence and morals.” Satcher Melinda’s daddy knew this; he had experienced it himself. The vast majority of underbites can be successfully treated at a very early age (Fig 2). Waiting for a poor
Journal of the American Orthodontic Society September-October 2011: Page 38