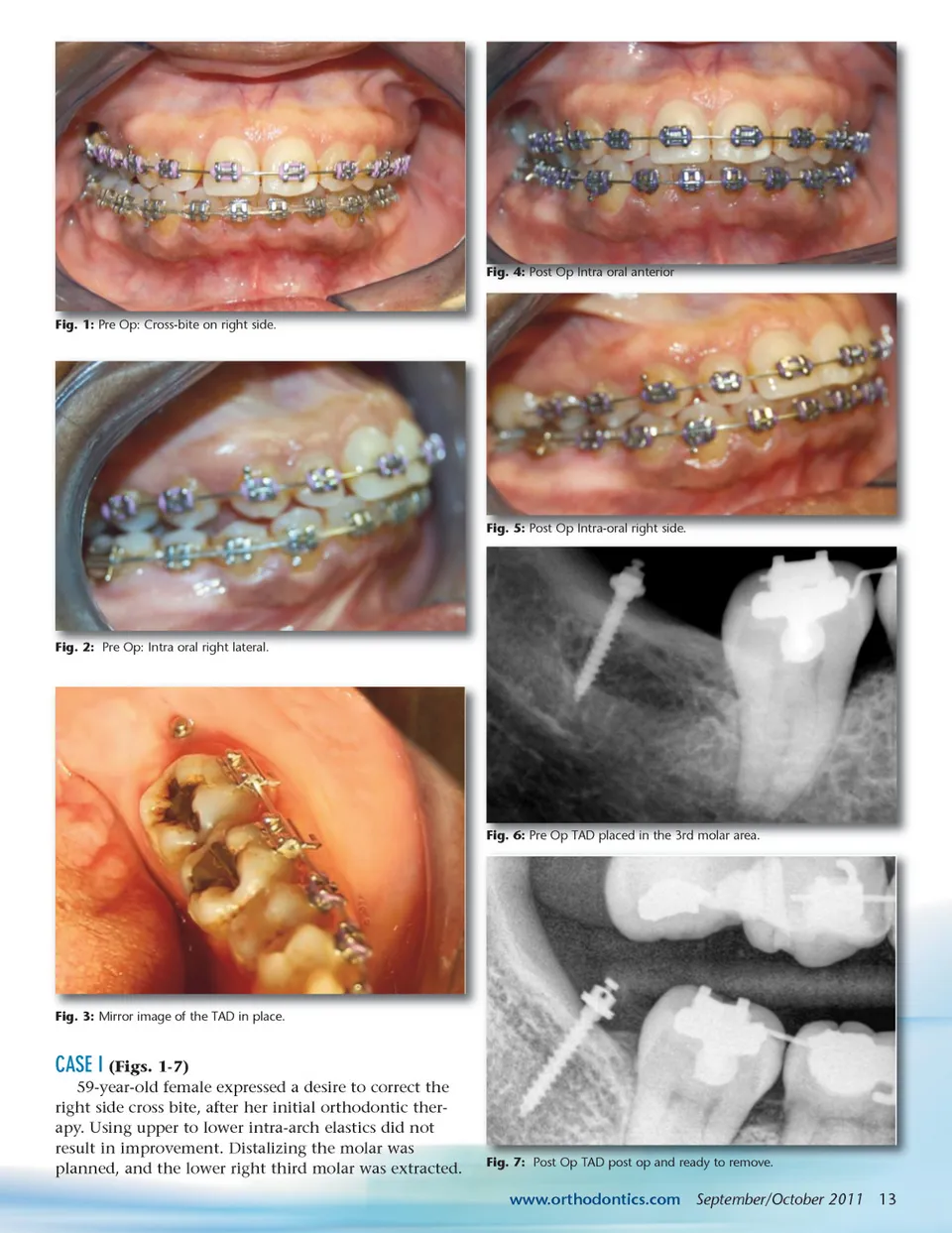
IMPROVING ANCHORAGE: TADs Use in Orthodontic Treatment Plans Deciding on which anchorage to use during orthodontic treatment plays a very important role in the final outcome. There are many intra-oral and extra-oral systems available, but most of them require patient compliance to prevent undesired tooth movement. Many of these undesired movements can be eliminated by the use of TADs. By Anilesh Katte, DDS, MAGD, Anuja Patel, BDS, MBA, Vikaskumar Patel, BDS, MBA, and Jim R. Prittinen, DDS emporary Anchorage Devices (TADs) are mini screws made of titanium. They are 1-to 2-mm in diameter and 6-to 12-mm in length. They are placed in the bone temporarily to improve orthodontic anchorage. 1 The use of temporary devices for skeletal anchorage was first proposed in 1945. 2 Since this introduction, TADs have gone through various changes in design and size. The U.S. Food and Drug Administration has given TADs its approval. 3 TADs have made it possible to almost totally eliminate the use of extra-oral headgear in many cases. Use of this mini screw technique can be applied, for example, in treatment of super-erupted molars. It also minimizes the need for patient compliance and thus increases the success of the orthodontic treatment. T In order to achieve successful temporary anchorage, proper site selection is critical. Placement of TADs in thick cortical bone gives more strength. 4 Even though TADs can be placed both bucally and palatally, it is necessary to take into account the patient’s growth phase. In growing patients, placement of TADs near the maxillary palatal suture site is contraindicated. 5, 6 Patients who are heavy smokers are poor candidates for the appli-cation of TADs. 7 Placing TADs in attached gingiva can eliminate soft tissue problems that sometimes occur when TADs are placed in mucobuccal gingiva. INDICATIONS í í í í Molar uprighting Molar intrusion Edentulous space closure Impacted canine: Either mesial or distal movement is possible í Forced eruption of unerupted teeth í Anterior open and deep bite correction. SITE SELECTION & PROCEDURE Temporary anchorage placement can be accom-plished as a minimally invasive procedure with just topical anesthesia. Local infiltration anesthesia and other methods of anesthesia can also be used if the clinician deems it necessary. TADs can be directly inserted through the gingiva. Various types of TADs are available, for example, self-drilling or self-tapping. Either one can be placed with the hand driver instru-ment provided with the kit. TADS are intended to be removed after completion of successful treatment. Removals of TAD are also done with use of a manual screwdriver tool provided with the kit. In order to eliminate any risk of swallow-ing the TAD, tying of the head of the screw with floss is recommended. 12 September/October 2011 JAOS CONTRAINDICATIONS í í í í í í Patient undergoing radiation therapy Presence of oral infection Heavy smokers History of metabolic disorders Diabetes, osteoporosis, osteomyelitis Poor periodontal support or presence of periodontitis í Poor bone support for placing mini implant
Journal of the American Orthodontic Society September-October 2011: Page 12