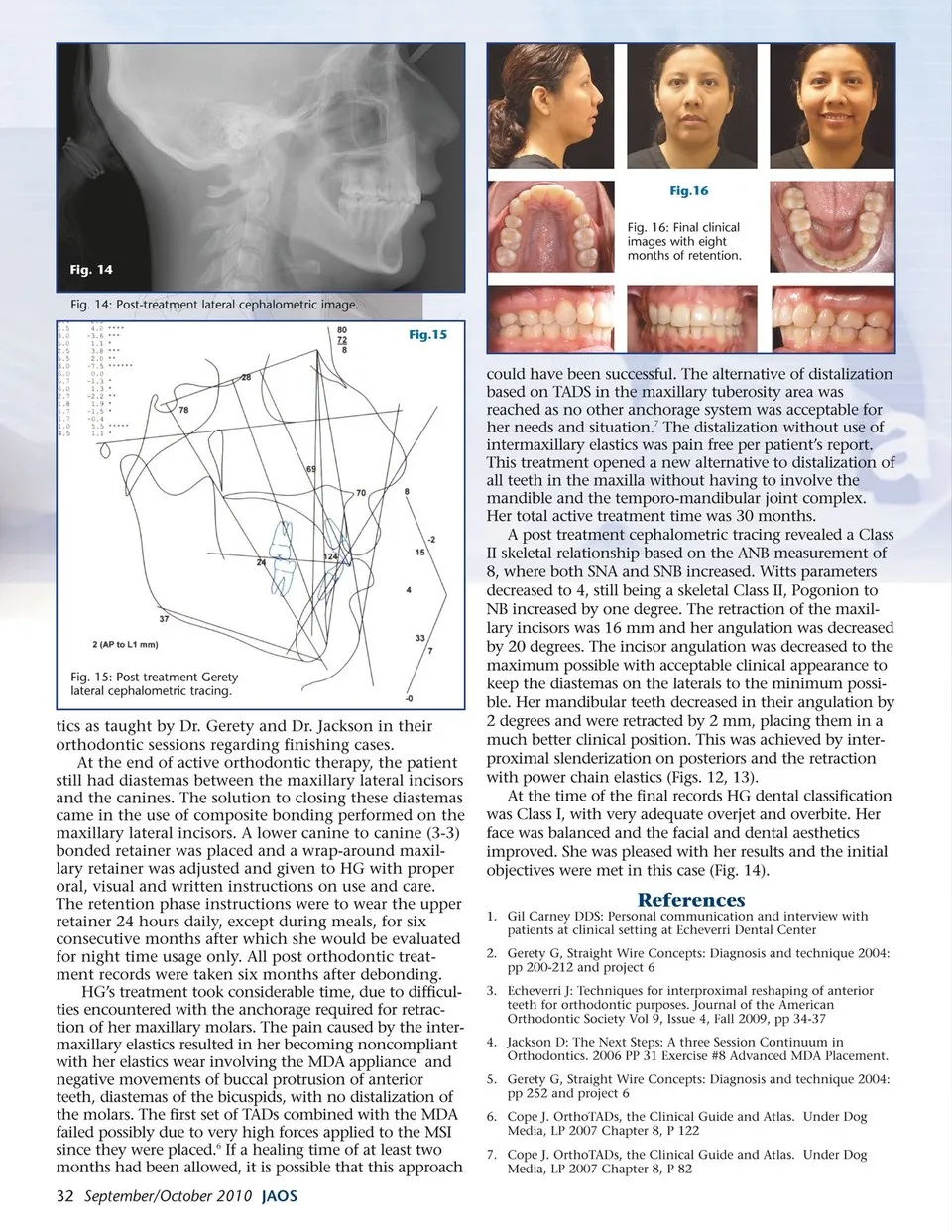
Fig.16 Fig. 16: Final clinical images with eight months of retention. Fig. 14 Fig. 14: Post-treatment lateral cephalometric image. Fig.15 could have been successful. The alternative of distalization based on TADS in the maxillary tuberosity area was reached as no other anchorage system was acceptable for her needs and situation.7 The distalization without use of Fig. 15: Post treatment Gerety lateral cephalometric tracing. tics as taught by Dr. Gerety and Dr. Jackson in their orthodontic sessions regarding finishing cases. At the end of active orthodontic therapy, the patient still had diastemas between the maxillary lateral incisors and the canines. The solution to closing these diastemas came in the use of composite bonding performed on the maxillary lateral incisors. A lower canine to canine (3-3) bonded retainer was placed and a wrap-around maxil-lary retainer was adjusted and given to HG with proper oral, visual and written instructions on use and care. The retention phase instructions were to wear the upper retainer 24 hours daily, except during meals, for six consecutive months after which she would be evaluated for night time usage only. All post orthodontic treat-ment records were taken six months after debonding. HG’s treatment took considerable time, due to difficul-ties encountered with the anchorage required for retrac-tion of her maxillary molars. The pain caused by the inter-maxillary elastics resulted in her becoming noncompliant with her elastics wear involving the MDA appliance and negative movements of buccal protrusion of anterior teeth, diastemas of the bicuspids, with no distalization of the molars. The first set of TADs combined with the MDA failed possibly due to very high forces applied to the MSI since they were placed.6 If a healing time of at least two months had been allowed, it is possible that this approach 32 September/October 2010 JAOS intermaxillary elastics was pain free per patient’s report. This treatment opened a new alternative to distalization of all teeth in the maxilla without having to involve the mandible and the temporo-mandibular joint complex. Her total active treatment time was 30 months. A post treatment cephalometric tracing revealed a Class II skeletal relationship based on the ANB measurement of 8, where both SNA and SNB increased. Witts parameters decreased to 4, still being a skeletal Class II, Pogonion to NB increased by one degree. The retraction of the maxil-lary incisors was 16 mm and her angulation was decreased by 20 degrees. The incisor angulation was decreased to the maximum possible with acceptable clinical appearance to keep the diastemas on the laterals to the minimum possi-ble. Her mandibular teeth decreased in their angulation by 2 degrees and were retracted by 2 mm, placing them in a much better clinical position. This was achieved by inter-proximal slenderization on posteriors and the retraction with power chain elastics (Figs. 12, 13). At the time of the final records HG dental classification was Class I, with very adequate overjet and overbite. Her face was balanced and the facial and dental aesthetics improved. She was pleased with her results and the initial objectives were met in this case (Fig. 14). References 1. Gil Carney DDS: Personal communication and interview with patients at clinical setting at Echeverri Dental Center 2. Gerety G, Straight Wire Concepts: Diagnosis and technique 2004: pp 200-212 and project 6 3. Echeverri J: Techniques for interproximal reshaping of anterior teeth for orthodontic purposes. Journal of the American Orthodontic Society Vol 9, Issue 4, Fall 2009, pp 34-37 4. Jackson D: The Next Steps: A three Session Continuum in Orthodontics. 2006 PP 31 Exercise #8 Advanced MDA Placement. 5. Gerety G, Straight Wire Concepts: Diagnosis and technique 2004: pp 252 and project 6 6. Cope J. OrthoTADs, the Clinical Guide and Atlas. Under Dog Media, LP 2007 Chapter 8, P 122 7. Cope J. OrthoTADs, the Clinical Guide and Atlas. Under Dog Media, LP 2007 Chapter 8, P 82
Journal of the American Orthodontic Society September-October 2010: Page 32