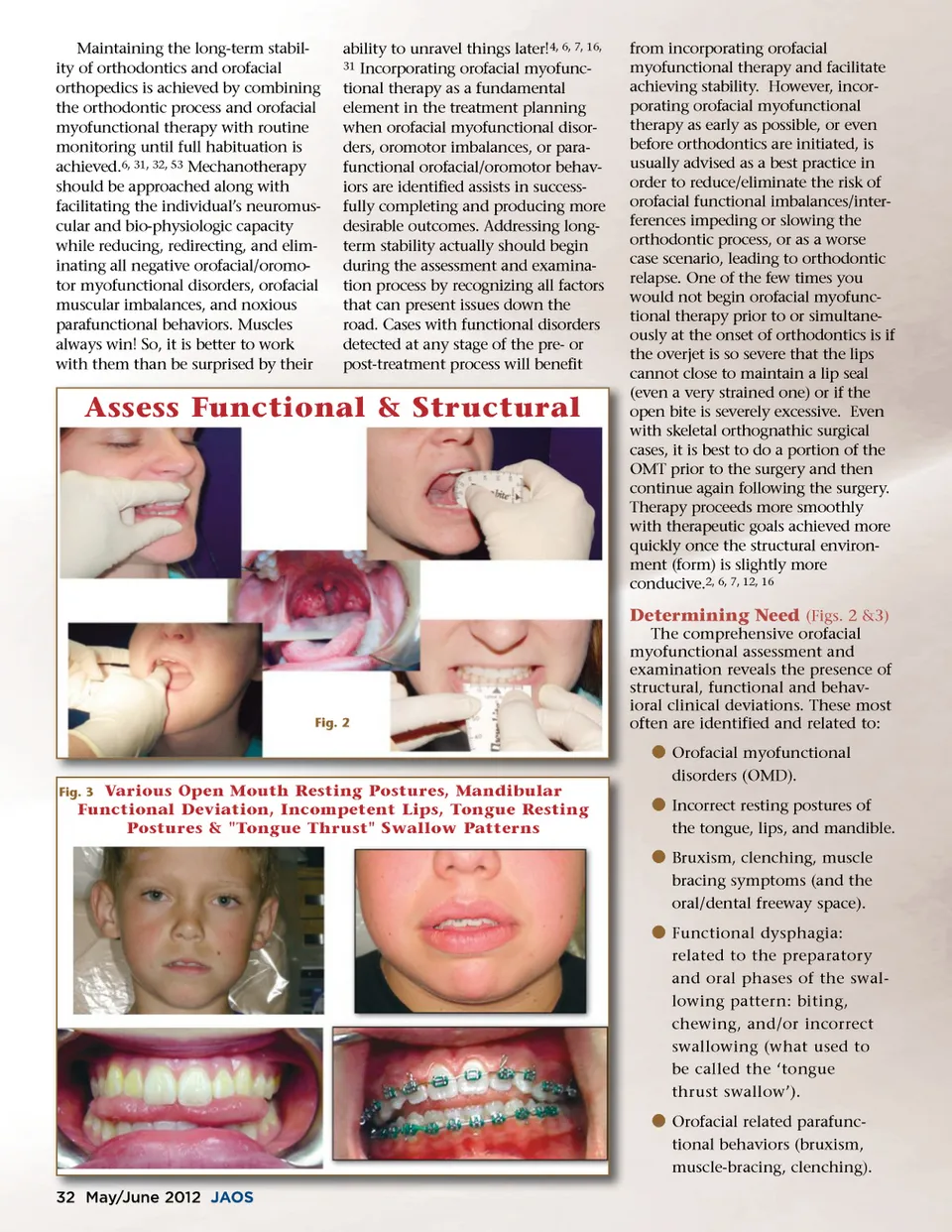
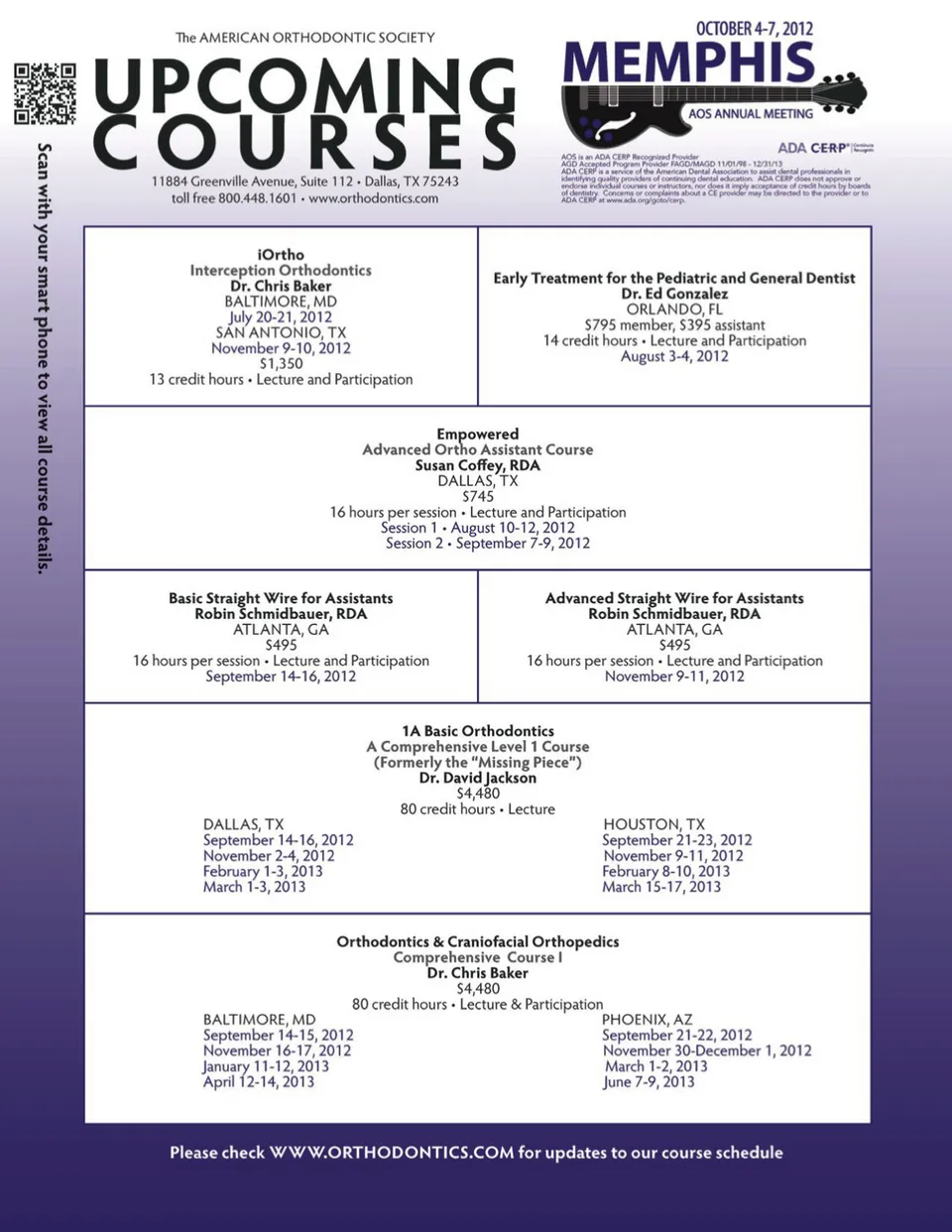
Maintaining the long-term stabil-ity of orthodontics and orofacial orthopedics is achieved by combining the orthodontic process and orofacial myofunctional therapy with routine monitoring until full habituation is achieved. 6, 31, 32, 53 Mechanotherapy should be approached along with facilitating the individual’s neuromus-cular and bio-physiologic capacity while reducing, redirecting, and elim-inating all negative orofacial/oromo-tor myofunctional disorders, orofacial muscular imbalances, and noxious parafunctional behaviors. Muscles always win! So, it is better to work with them than be surprised by their ability to unravel things later! 4, 6, 7, 16, 31 Incorporating orofacial myofunc-tional therapy as a fundamental element in the treatment planning when orofacial myofunctional disor-ders, oromotor imbalances, or para-functional orofacial/oromotor behav-iors are identified assists in success-fully completing and producing more desirable outcomes. Addressing long-term stability actually should begin during the assessment and examina-tion process by recognizing all factors that can present issues down the road. Cases with functional disorders detected at any stage of the pre-or post-treatment process will benefit Assess Functional & Structural from incorporating orofacial myofunctional therapy and facilitate achieving stability. However, incor-porating orofacial myofunctional therapy as early as possible, or even before orthodontics are initiated, is usually advised as a best practice in order to reduce/eliminate the risk of orofacial functional imbalances/inter-ferences impeding or slowing the orthodontic process, or as a worse case scenario, leading to orthodontic relapse. One of the few times you would not begin orofacial myofunc-tional therapy prior to or simultane-ously at the onset of orthodontics is if the overjet is so severe that the lips cannot close to maintain a lip seal (even a very strained one) or if the open bite is severely excessive. Even with skeletal orthognathic surgical cases, it is best to do a portion of the OMT prior to the surgery and then continue again following the surgery. Therapy proceeds more smoothly with therapeutic goals achieved more quickly once the structural environ-ment (form) is slightly more conducive. 2, 6, 7, 12, 16 Determining Need (Figs. 2 &3) The comprehensive orofacial myofunctional assessment and examination reveals the presence of structural, functional and behav-ioral clinical deviations. These most often are identified and related to: Fig. 2 b Orofacial myofunctional disorders (OMD). Fig. 3 Various Open Mouth Resting Postures, Mandibular Functional Deviation, Incompetent Lips, Tongue Resting Postures & "Tongue Thrust" Swallow Patterns b Incorrect resting postures of the tongue, lips, and mandible. b Bruxism, clenching, muscle bracing symptoms (and the oral/dental freeway space). b Functional dysphagia: related to the preparatory and oral phases of the swal-lowing pattern: biting, chewing, and/or incorrect swallowing (what used to be called the ‘tongue thrust swallow’). b Orofacial related parafunc-tional behaviors (bruxism, muscle-bracing, clenching). 32 May/June May/ y / J une 2012 J JAOS AOS
Journal of the American Orthodontic Society May-June 2012: Page 32