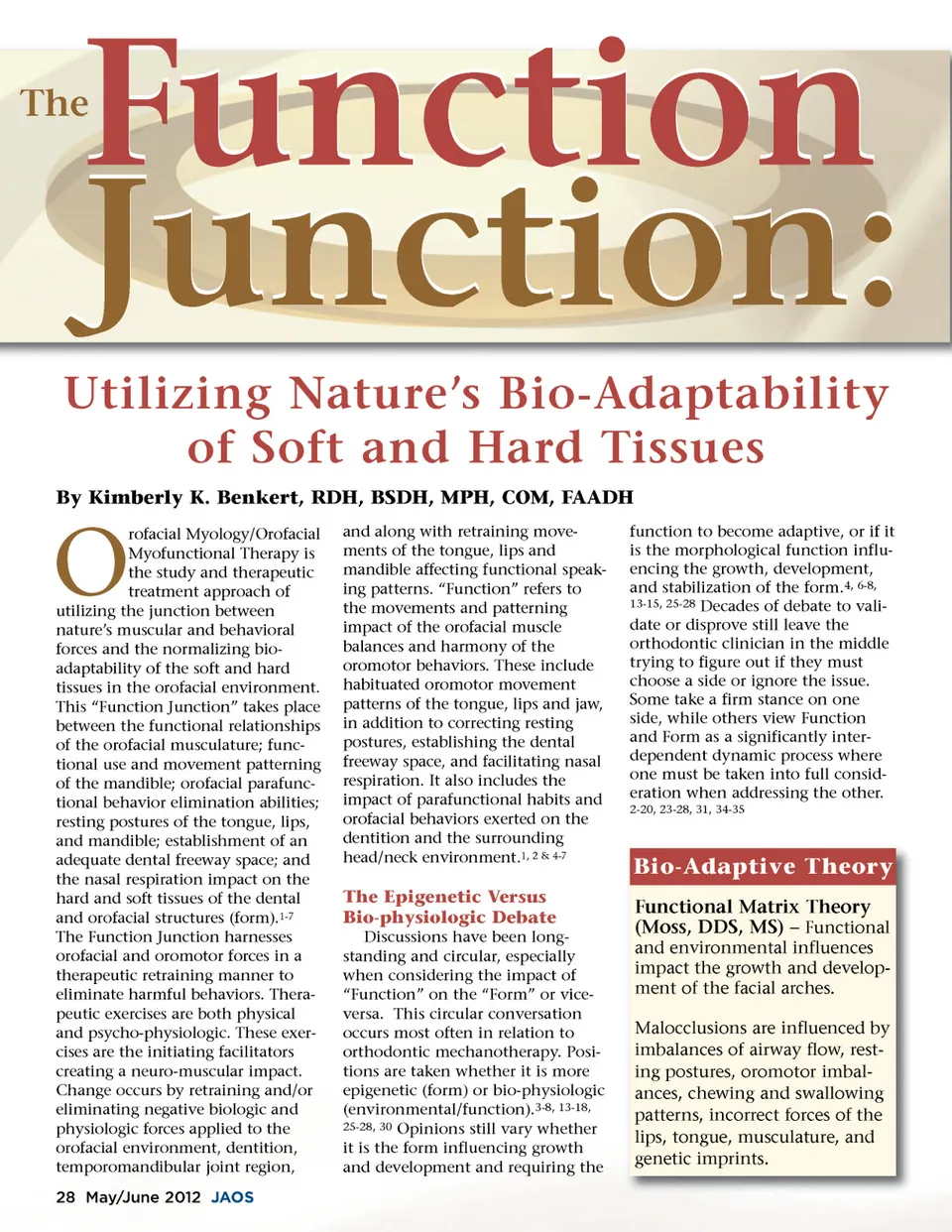
Regardless of one’s initial stance, hopefully the question of how the function impacts the form (and vice versa) is considered and incorpo-rated into the critical decision making process with each orthodontic case. The challenge facing orthodontic clinicians is using evidence-based research along with individualized patient treat-ment goals to establish a harmo-nious interplay between the func-tion, form, orthodontics, and ortho-pedic therapy…. and having it last! 6, 21 Anatomist, Harry Sicher, advocated the importance of “Normalizing the intricate balance between the teeth, skeletal and muscular system”. 7 Sicher describes creating a balance that includes establishing and maintaining a dental (oral) freeway space. A dental (oral) freeway space is the mandibu-lar resting posture maintaining a 2-3 mm posterior (molar) inter-dental (inter-occlusal) space with approxi-mately 4-5 mm maintained in the anterior (incisal). When the mandible sits in its physiologic rest-ing posture, the tongue is resting on the palate (Fig.1) with the dental freeway space maintained and the lips lightly closed at rest. A balanced equilibrium is reached between the external forces of the lips, facial and masticatory muscula-ture against the dentition and the internal resting posture of the tongue against the palate while normal nasal respiration takes place. Maintaining the dental free-way space allows the uninterrupted physiologic eruption of the teeth. He conveyed that clinicians need to become biological anatomists and more fully take the biologic-physio-logic systems into account during treatment. 6, 7 issues creating the negative environ-mental impact. The literature indi-cates a clear need to incorporate functional issues and include treat-ment for orofacial myofunctional disorders in order to be able to create the ideal occlusion, and then maintain its stability within the orofacial and dental environment over the long-term. The scientific evidence depicting function signifi-cantly impacting form continues to build through the literature. 4-8,10, 16, 25-29, 32, 53 Orthodontic practition-ers’ attitudes are also moving towards using evidence-based diag-nosis and treatment more frequently to assist with their clini-cal decision-making processes. 21, 22 Utilizing an evidence-based approach to address the interrela-tionship between function and form diminishes the debate, even among skeptics. Lingual-Palatal Tongue Rest Posture (The Spot) Fig. 1 manner. Moss states one cannot separate the environmental (muscu-lar and behavioral) impact on the structural (epigenetic form), and vice versa. 25-28 Kondo demonstrates cases, followed for 25 years, retain their orthodontic corrective integrity when coupled with orofa-cial myofunctional therapies. 6 History and Scope of Care Individuals have been address-ing orofacial/oromotor dysfunction with orofacial muscle exercise since the early 1900’s. Providing a program of therapeutics became better known in the 1950’s through Walter Straub’s efforts, and became an organized specialty focus in the1970’s through the organizational formation of the International Association of Orofa-cial Myology (IAOM). 2, 4, 6, 7, 9-12, 16, 19-20, 35-40 An interdisciplinary team approach keeps the patient at the center of all of the treatment modalities and leads to the most stable outcomes. 2, 6, 12, 16, 53 A disparity exists in the number of certified orofacial myologists in comparison to the numbers of individuals who would benefit from potential treatment.This poses a significant dilemma for orthodon-tists not in close proximity to an orofacial myologist. Leaving orofa-cial myofunctional disorders untreated increases the risk factors for orthodontic relapse. A bigger dilemma exists when the orofacial myofunctional disorders remain unnoticed and referral is non-exis-tent. For the practitioner observing and recognizing dysfunction and then taking no action, it places the practitioner in an ethical, moral, and potential legal dilemma. 48, 49, 50 In the scenario of non-recogni-tion, it places the practitioner in an even more vulnerable clinical liability position for potential relapse. 6, 7, 31, 53, 54 Based on experi-ence levels, some orofacial myolo-gists are capable of offering tele-therapy via video conferencing with patients unable to travel to a therapist’s office. It is an excellent therapeutic option for practitioners without an orofacial myologist in the immediate area. Moving Forward Based on Evidence Scholars support and recognize maintaining normalized function is challenging if orofacial or oromotor dysfunction is present. Orofacial myology is a treatment considera-tion that fits nicely with orthodon-tics. Orofacial Myofunctional Ther-apy methodologies address the orofacial and oromotor functional The three decades h last l h d d of f support-ing evidence in the literature shifts from debate towards discussions of how to best deal with negative func-tional impacts. 2, 5, 6, 12, 16, 29-32, 34, 42-47, 53 This requires a paradigm shift for some practitioners in their thoughts and treatment processes. It becomes easier to understand as multiple sources in dentistry and medicine continue adding to the clinical and behavioral evidence documenting that orofacial myofunctional therapies serve as preventive, interceptive and thera-peutic interventions. 1, 2, 5, 6, 16, 24, 31, 53, 54 Theories present that separa-tion of the two philosophies of “Function VS Form” and “Form VS Function” is not only difficult, but actually unwise to ignore in clinical practice. Moss’ Functional Matrix Theory provides added support to the inter-relational dependence focused in a multi-dimensional www.orthodontics.com May/June 2012 29
Journal of the American Orthodontic Society May-June 2012: Page 29