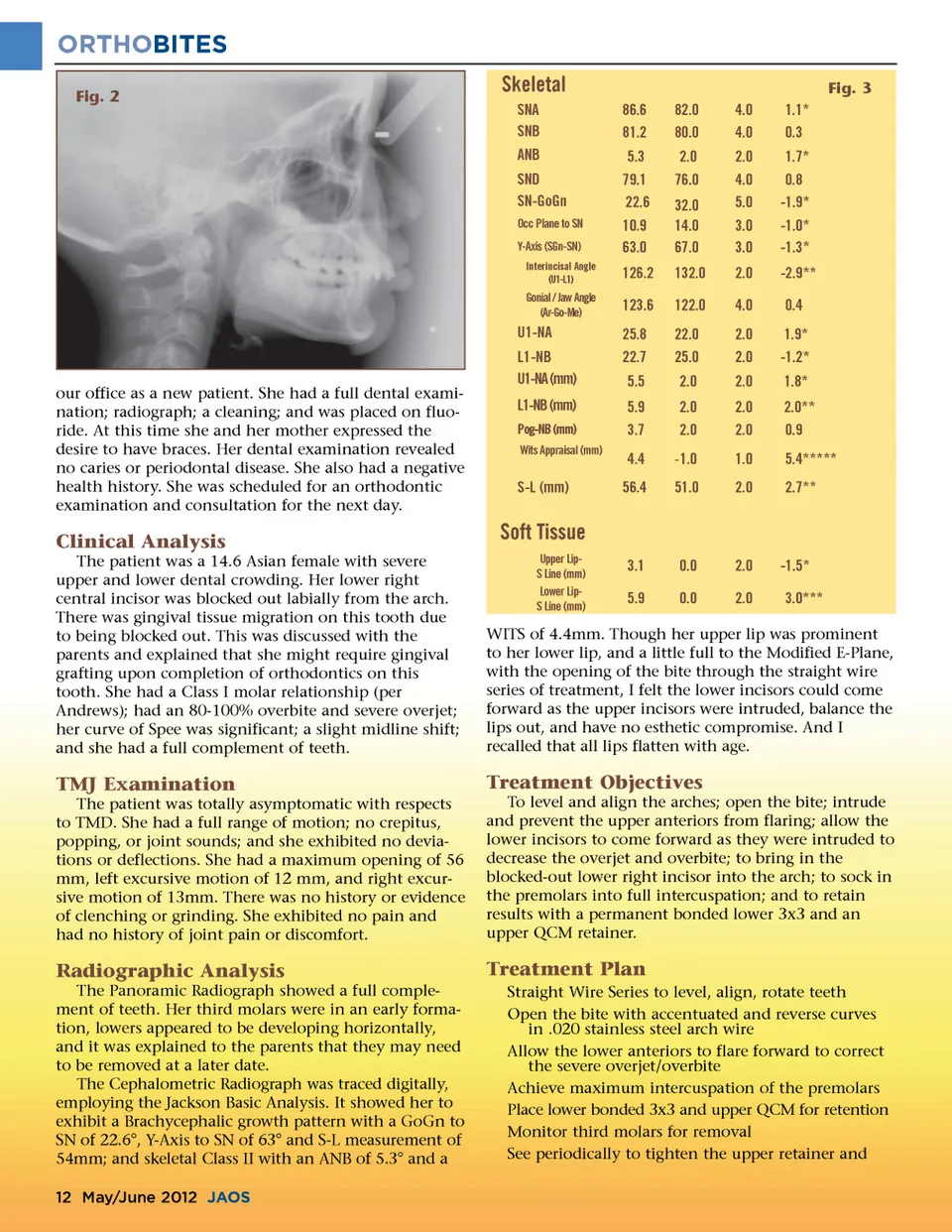
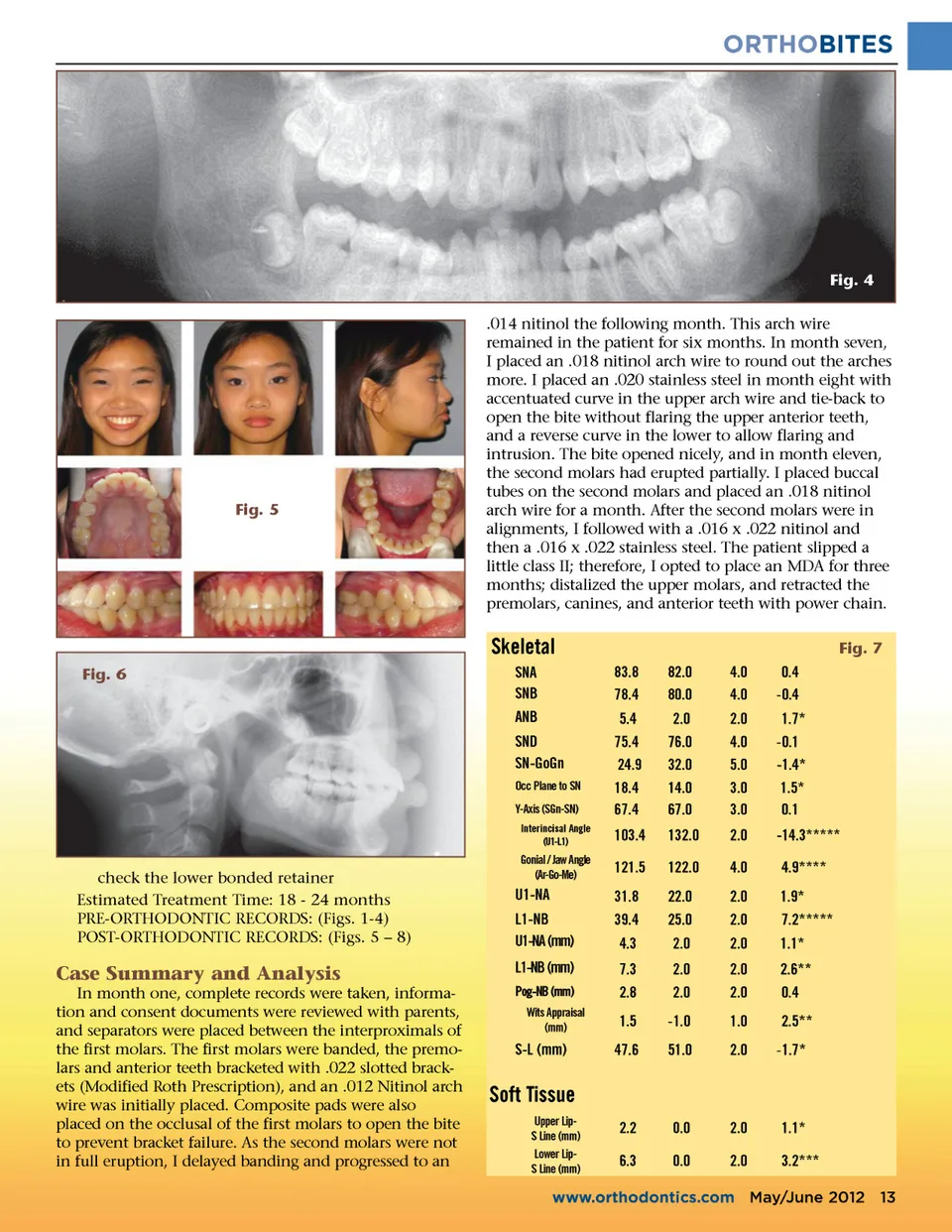
ORTHOBITES Fig. 2 Skeletal SNA SNB ANB SND SN-GoGn Occ Plane to SN Y-Axis (SGn-SN) Interincisal Angle (U1-L1) Fig. 3 86.6 81.2 5.3 79.1 22.6 10.9 63.0 126.2 123.6 25.8 22.7 5.5 5.9 3.7 4.4 56.4 82.0 80.0 2.0 76.0 32.0 14.0 67.0 132.0 122.0 22.0 25.0 2.0 2.0 2.0 -1.0 51.0 4.0 4.0 2.0 4.0 5.0 3.0 3.0 2.0 4.0 2.0 2.0 2.0 2.0 2.0 1.0 2.0 1.1* 0.3 1.7* 0.8 -1.9* -1.0* -1.3* -2.9** 0.4 1.9* -1.2* 1.8* 2.0** 0.9 5.4***** 2.7** Gonial / Jaw Angle (Ar-Go-Me) U1-NA L1-NB U1-NA (mm) our office as a new patient. She had a full dental exami-nation; radiograph; a cleaning; and was placed on fluo-ride. At this time she and her mother expressed the desire to have braces. Her dental examination revealed no caries or periodontal disease. She also had a negative health history. She was scheduled for an orthodontic examination and consultation for the next day. L1-NB (mm) Pog-NB (mm) Wits Appraisal (mm) S-L (mm) Clinical Analysis The patient was a 14.6 Asian female with severe upper and lower dental crowding. Her lower right central incisor was blocked out labially from the arch. There was gingival tissue migration on this tooth due to being blocked out. This was discussed with the parents and explained that she might require gingival grafting upon completion of orthodontics on this tooth. She had a Class I molar relationship (per Andrews); had an 80-100% overbite and severe overjet; her curve of Spee was significant; a slight midline shift; and she had a full complement of teeth. Soft Tissue Upper Lip-S Line (mm) Lower Lip-S Line (mm) 3.1 5.9 0.0 0.0 2.0 2.0 -1.5* 3.0*** WITS of 4.4mm. Though her upper lip was prominent to her lower lip, and a little full to the Modified E-Plane, with the opening of the bite through the straight wire series of treatment, I felt the lower incisors could come forward as the upper incisors were intruded, balance the lips out, and have no esthetic compromise. And I recalled that all lips flatten with age. TMJ Examination The patient was totally asymptomatic with respects to TMD. She had a full range of motion; no crepitus, popping, or joint sounds; and she exhibited no devia-tions or deflections. She had a maximum opening of 56 mm, left excursive motion of 12 mm, and right excur-sive motion of 13mm. There was no history or evidence of clenching or grinding. She exhibited no pain and had no history of joint pain or discomfort. Treatment Objectives To level and align the arches; open the bite; intrude and prevent the upper anteriors from flaring; allow the lower incisors to come forward as they were intruded to decrease the overjet and overbite; to bring in the blocked-out lower right incisor into the arch; to sock in the premolars into full intercuspation; and to retain results with a permanent bonded lower 3x3 and an upper QCM retainer. Radiographic Analysis The Panoramic Radiograph showed a full comple-ment of teeth. Her third molars were in an early forma-tion, lowers appeared to be developing horizontally, and it was explained to the parents that they may need to be removed at a later date. The Cephalometric Radiograph was traced digitally, employing the Jackson Basic Analysis. It showed her to exhibit a Brachycephalic growth pattern with a GoGn to SN of 22.6°, Y-Axis to SN of 63° and S-L measurement of 54mm; and skeletal Class II with an ANB of 5.3° and a 12 May/June 2012 JAOS Treatment Plan Straight Wire Series to level, align, rotate teeth Open the bite with accentuated and reverse curves in .020 stainless steel arch wire Allow the lower anteriors to flare forward to correct the severe overjet/overbite Achieve maximum intercuspation of the premolars Place lower bonded 3x3 and upper QCM for retention Monitor third molars for removal See periodically to tighten the upper retainer and
Journal of the American Orthodontic Society May-June 2012: Page 12