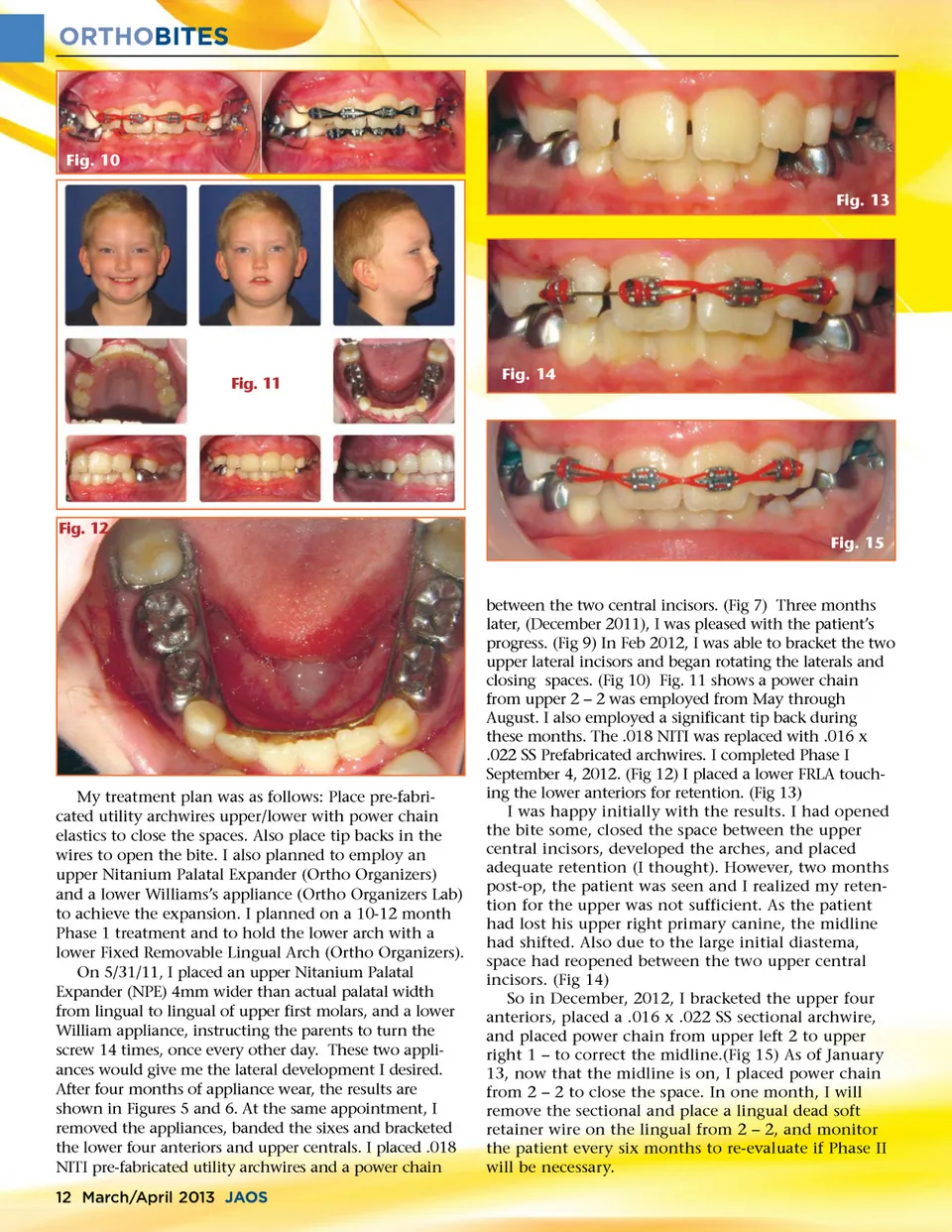
ORTHOBITES Fig. 10 Fig. 13 Fig. 11 Fig. 14 Fig. 12 Fig. 15 My treatment plan was as follows: Place pre-fabri-cated utility archwires upper/lower with power chain elastics to close the spaces. Also place tip backs in the wires to open the bite. I also planned to employ an upper Nitanium Palatal Expander (Ortho Organizers) and a lower Williams’s appliance (Ortho Organizers Lab) to achieve the expansion. I planned on a 10-12 month Phase 1 treatment and to hold the lower arch with a lower Fixed Removable Lingual Arch (Ortho Organizers). On 5/31/11, I placed an upper Nitanium Palatal Expander (NPE) 4mm wider than actual palatal width from lingual to lingual of upper first molars, and a lower William appliance, instructing the parents to turn the screw 14 times, once every other day. These two appli-ances would give me the lateral development I desired. After four months of appliance wear, the results are shown in Figures 5 and 6. At the same appointment, I removed the appliances, banded the sixes and bracketed the lower four anteriors and upper centrals. I placed .018 NITI pre-fabricated utility archwires and a power chain 12 March/April 2013 JAOS between the two central incisors. (Fig 7) Three months later, (December 2011), I was pleased with the patient’s progress. (Fig 9) In Feb 2012, I was able to bracket the two upper lateral incisors and began rotating the laterals and closing spaces. (Fig 10) Fig. 11 shows a power chain from upper 2 – 2 was employed from May through August. I also employed a significant tip back during these months. The .018 NITI was replaced with .016 x .022 SS Prefabricated archwires. I completed Phase I September 4, 2012. (Fig 12) I placed a lower FRLA touch-ing the lower anteriors for retention. (Fig 13) I was happy initially with the results. I had opened the bite some, closed the space between the upper central incisors, developed the arches, and placed adequate retention (I thought). However, two months post-op, the patient was seen and I realized my reten-tion for the upper was not sufficient. As the patient had lost his upper right primary canine, the midline had shifted. Also due to the large initial diastema, space had reopened between the two upper central incisors. (Fig 14) So in December, 2012, I bracketed the upper four anteriors, placed a .016 x .022 SS sectional archwire, and placed power chain from upper left 2 to upper right 1 – to correct the midline.(Fig 15) As of January 13, now that the midline is on, I placed power chain from 2 – 2 to close the space. In one month, I will remove the sectional and place a lingual dead soft retainer wire on the lingual from 2 – 2, and monitor the patient every six months to re-evaluate if Phase II will be necessary.
Journal of the American Orthodontic Society March-April 2013: Page 12