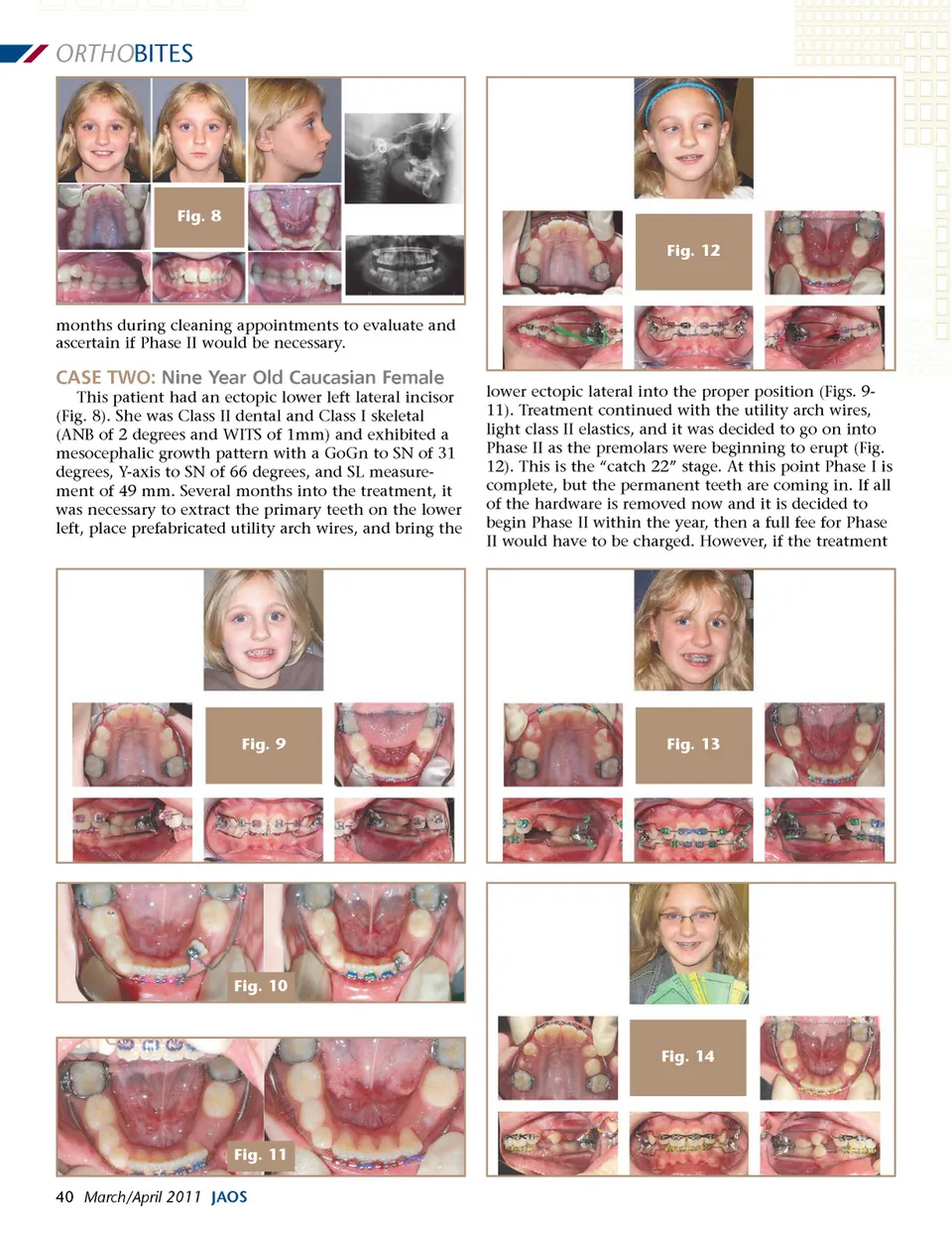
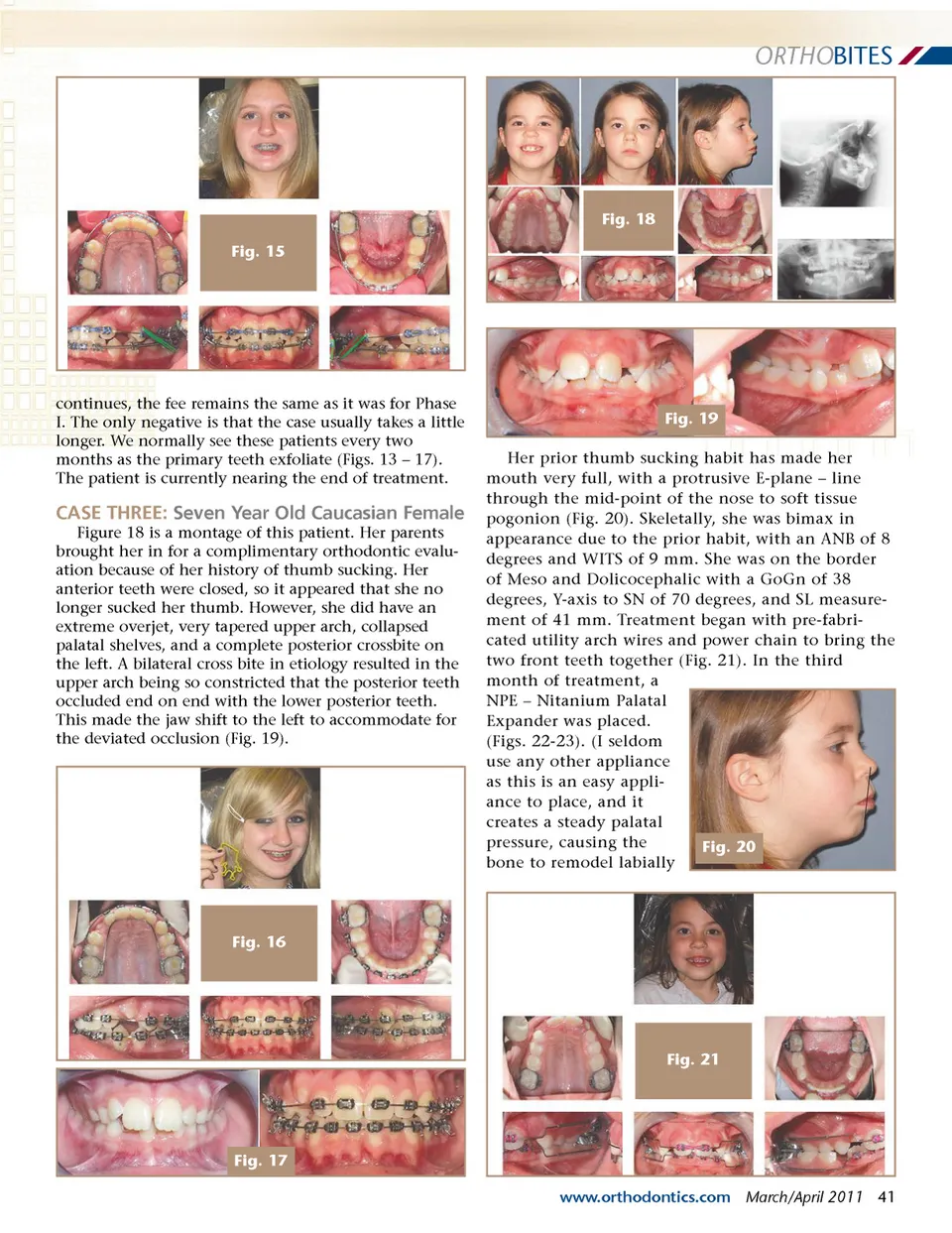
ORTHO BITES Fig. 18 Fig. 15 continues, the fee remains the same as it was for Phase I. The only negative is that the case usually takes a little longer. We normally see these patients every two months as the primary teeth exfoliate (Figs. 13 – 17). The patient is currently nearing the end of treatment. Fig. 19 Her prior thumb sucking habit has made her mouth very full, with a protrusive E-plane – line through the mid-point of the nose to soft tissue pogonion (Fig. 20). Skeletally, she was bimax in appearance due to the prior habit, with an ANB of 8 degrees and WITS of 9 mm. She was on the border of Meso and Dolicocephalic with a GoGn of 38 degrees, Y-axis to SN of 70 degrees, and SL measure-ment of 41 mm. Treatment began with pre-fabri-cated utility arch wires and power chain to bring the two front teeth together (Fig. 21). In the third month of treatment, a NPE – Nitanium Palatal Expander was placed. (Figs. 22-23). (I seldom use any other appliance as this is an easy appli-ance to place, and it creates a steady palatal pressure, causing the Fig. 20 bone to remodel labially CASE THREE: Seven Year Old Caucasian Female Figure 18 is a montage of this patient. Her parents brought her in for a complimentary orthodontic evalu-ation because of her history of thumb sucking. Her anterior teeth were closed, so it appeared that she no longer sucked her thumb. However, she did have an extreme overjet, very tapered upper arch, collapsed palatal shelves, and a complete posterior crossbite on the left. A bilateral cross bite in etiology resulted in the upper arch being so constricted that the posterior teeth occluded end on end with the lower posterior teeth. This made the jaw shift to the left to accommodate for the deviated occlusion (Fig. 19). Fig. 16 Fig. 21 Fig. 17 www.orthodontics.com March/April 2011 41
Journal of the American Orthodontic Society March-April 2011: Page 41