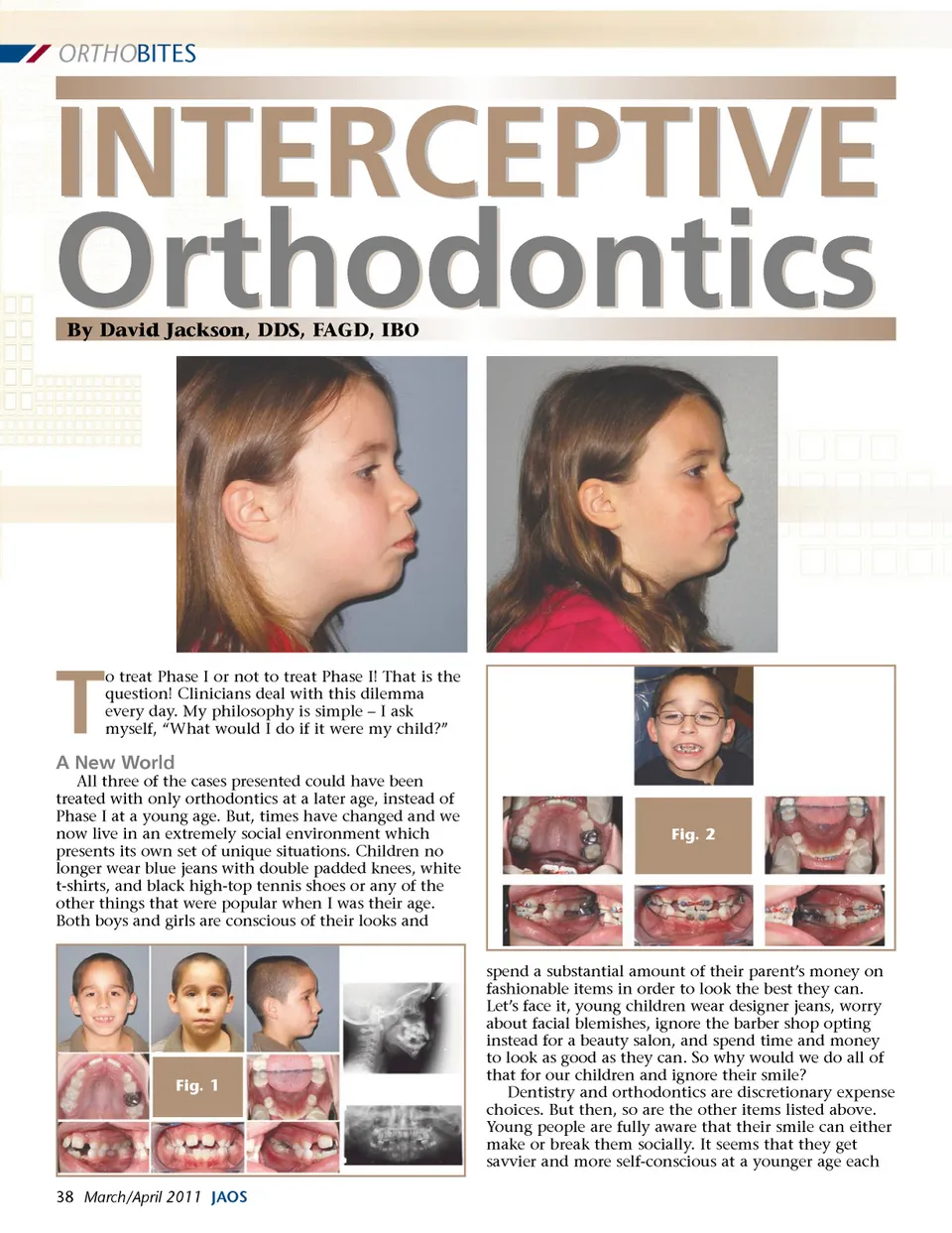
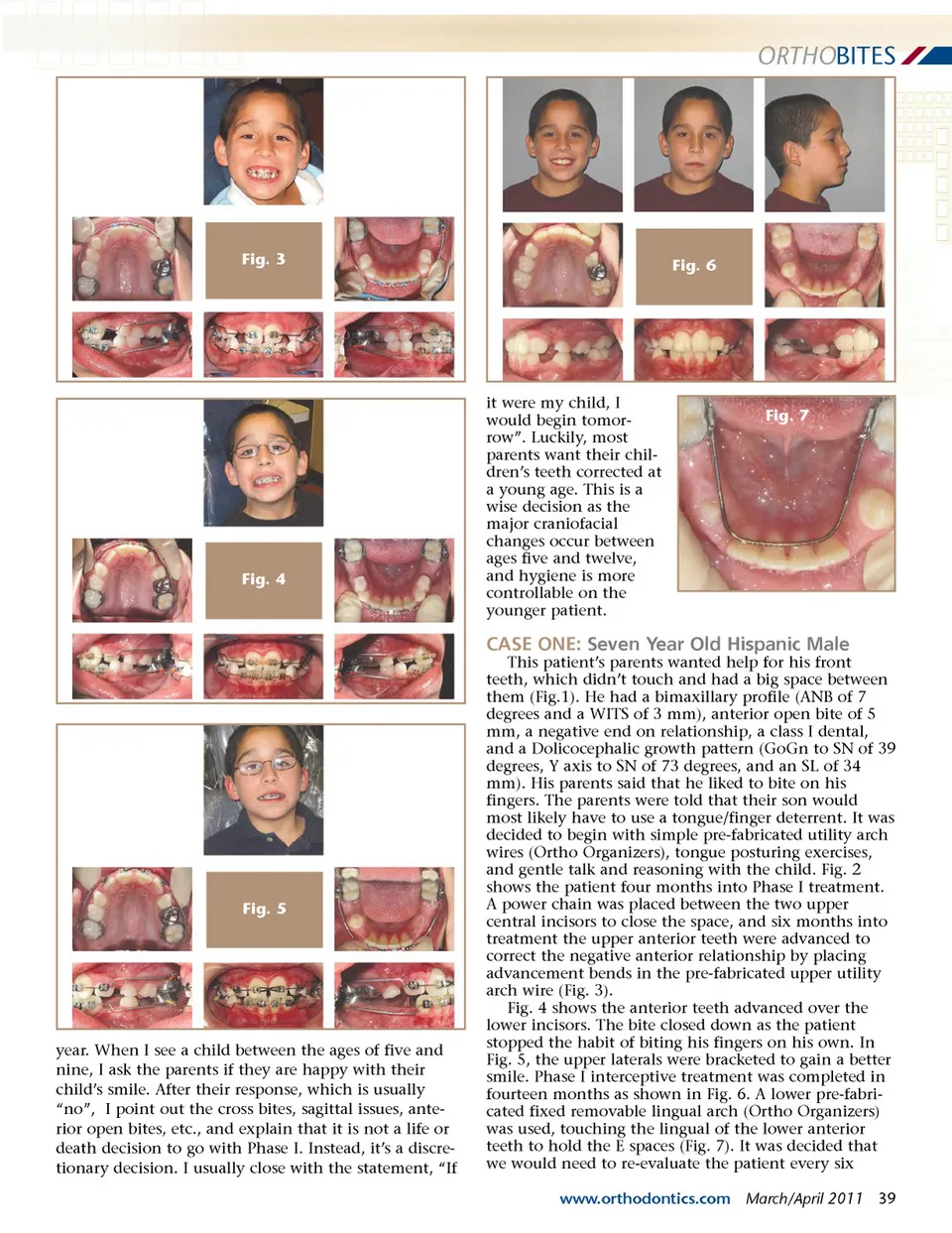
ORTHO BITES Fig. 3 Fig. 6 Fig. 4 it were my child, I would begin tomor-row”. Luckily, most parents want their chil-dren’s teeth corrected at a young age. This is a wise decision as the major craniofacial changes occur between ages five and twelve, and hygiene is more controllable on the younger patient. Fig. 7 CASE ONE: Seven Year Old Hispanic Male This patient’s parents wanted help for his front teeth, which didn’t touch and had a big space between them (Fig.1). He had a bimaxillary profile (ANB of 7 degrees and a WITS of 3 mm), anterior open bite of 5 mm, a negative end on relationship, a class I dental, and a Dolicocephalic growth pattern (GoGn to SN of 39 degrees, Y axis to SN of 73 degrees, and an SL of 34 mm). His parents said that he liked to bite on his fingers. The parents were told that their son would most likely have to use a tongue/finger deterrent. It was decided to begin with simple pre-fabricated utility arch wires (Ortho Organizers), tongue posturing exercises, and gentle talk and reasoning with the child. Fig. 2 shows the patient four months into Phase I treatment. A power chain was placed between the two upper central incisors to close the space, and six months into treatment the upper anterior teeth were advanced to correct the negative anterior relationship by placing advancement bends in the pre-fabricated upper utility arch wire (Fig. 3). Fig. 4 shows the anterior teeth advanced over the lower incisors. The bite closed down as the patient stopped the habit of biting his fingers on his own. In Fig. 5, the upper laterals were bracketed to gain a better smile. Phase I interceptive treatment was completed in fourteen months as shown in Fig. 6. A lower pre-fabri-cated fixed removable lingual arch (Ortho Organizers) was used, touching the lingual of the lower anterior teeth to hold the E spaces (Fig. 7). It was decided that we would need to re-evaluate the patient every six www.orthodontics.com March/April 2011 39 Fig. 5 year. When I see a child between the ages of five and nine, I ask the parents if they are happy with their child’s smile. After their response, which is usually “no”, I point out the cross bites, sagittal issues, ante-rior open bites, etc., and explain that it is not a life or death decision to go with Phase I. Instead, it’s a discre-tionary decision. I usually close with the statement, “If
Journal of the American Orthodontic Society March-April 2011: Page 39