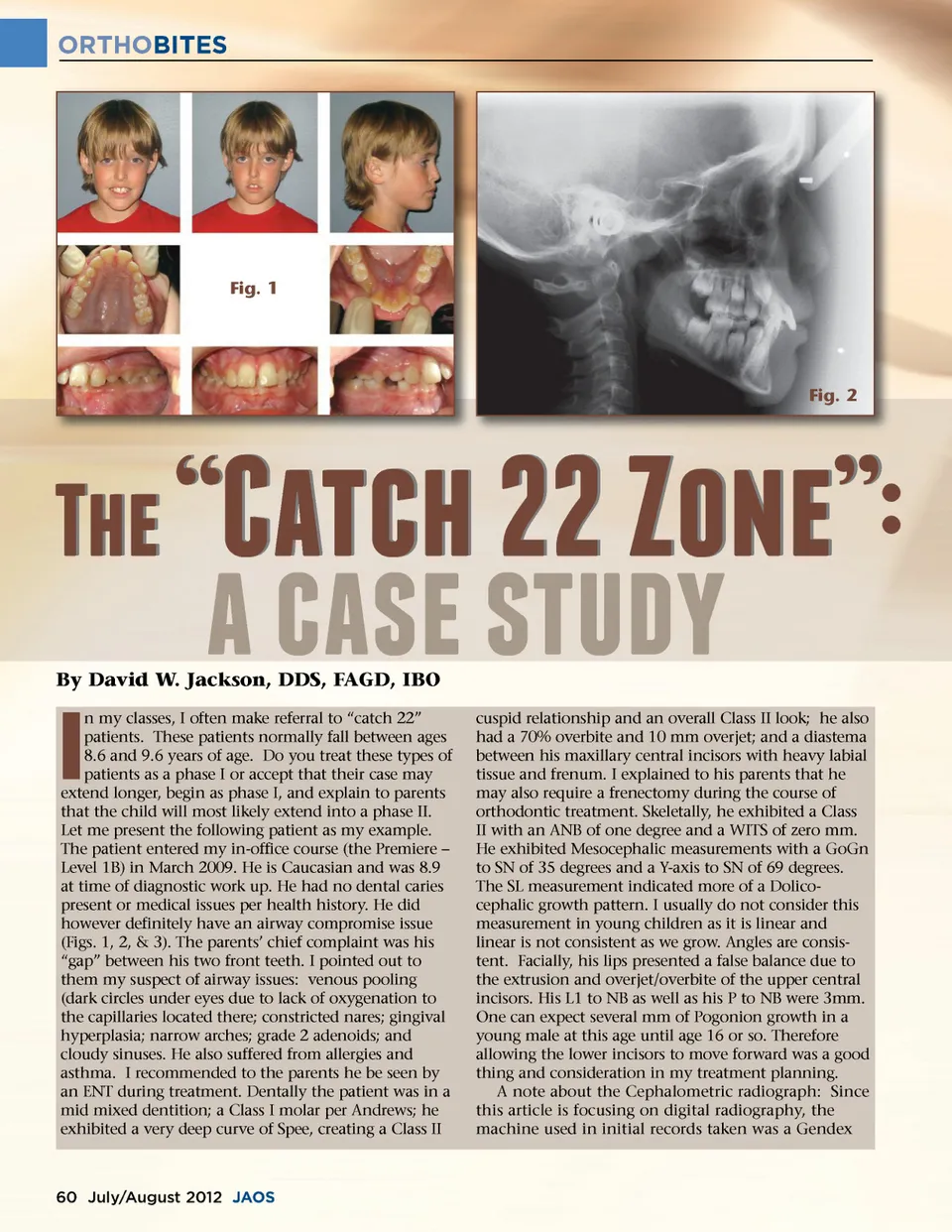
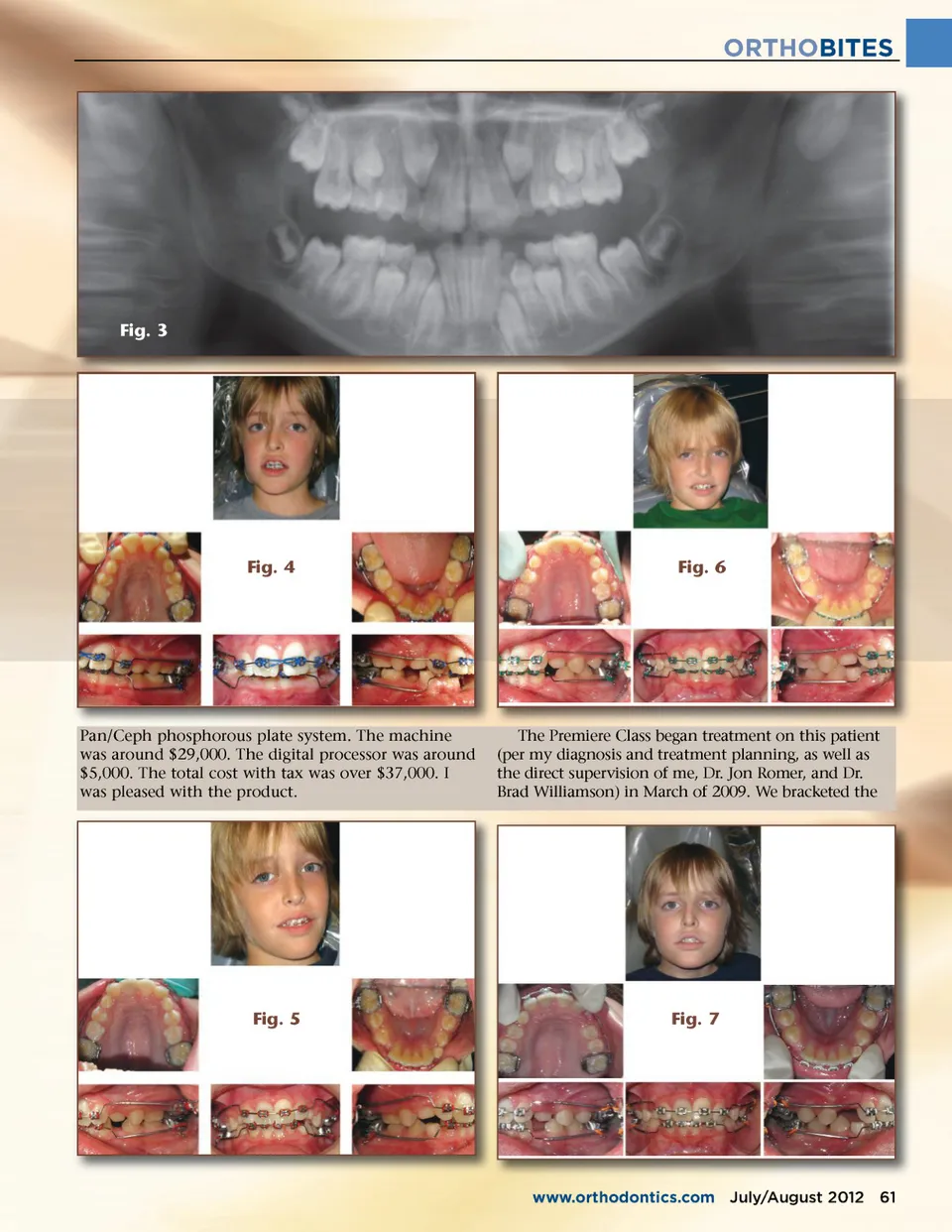
ORTHOBITES Fig. 1 Fig. 2 �a;f;#$ �c;!"f;$$e; By David W. Jackson, DDS, FAGD, IBO !$!b;#$b;"a; # # n my classes, I often make referral to “catch 22” patients. These patients normally fall between ages 8.6 and 9.6 years of age. Do you treat these types of patients as a phase I or accept that their case may extend longer, begin as phase I, and explain to parents that the child will most likely extend into a phase II. Let me present the following patient as my example. The patient entered my in-office course (the Premiere – Level 1B) in March 2009. He is Caucasian and was 8.9 at time of diagnostic work up. He had no dental caries present or medical issues per health history. He did however definitely have an airway compromise issue (Figs. 1, 2, & 3). The parents’ chief complaint was his “gap” between his two front teeth. I pointed out to them my suspect of airway issues: venous pooling (dark circles under eyes due to lack of oxygenation to the capillaries located there; constricted nares; gingival hyperplasia; narrow arches; grade 2 adenoids; and cloudy sinuses. He also suffered from allergies and asthma. I recommended to the parents he be seen by an ENT during treatment. Dentally the patient was in a mid mixed dentition; a Class I molar per Andrews; he exhibited a very deep curve of Spee, creating a Class II I cuspid relationship and an overall Class II look; he also had a 70% overbite and 10 mm overjet; and a diastema between his maxillary central incisors with heavy labial tissue and frenum. I explained to his parents that he may also require a frenectomy during the course of orthodontic treatment. Skeletally, he exhibited a Class II with an ANB of one degree and a WITS of zero mm. He exhibited Mesocephalic measurements with a GoGn to SN of 35 degrees and a Y-axis to SN of 69 degrees. The SL measurement indicated more of a Dolico-cephalic growth pattern. I usually do not consider this measurement in young children as it is linear and linear is not consistent as we grow. Angles are consis-tent. Facially, his lips presented a false balance due to the extrusion and overjet/overbite of the upper central incisors. His L1 to NB as well as his P to NB were 3mm. One can expect several mm of Pogonion growth in a young male at this age until age 16 or so. Therefore allowing the lower incisors to move forward was a good thing and consideration in my treatment planning. A note about the Cephalometric radiograph: Since this article is focusing on digital radiography, the machine used in initial records taken was a Gendex 60 July/August 2012 JAOS
Journal of the American Orthodontic Society July-August 2012 Buyer's Guide: Page 60