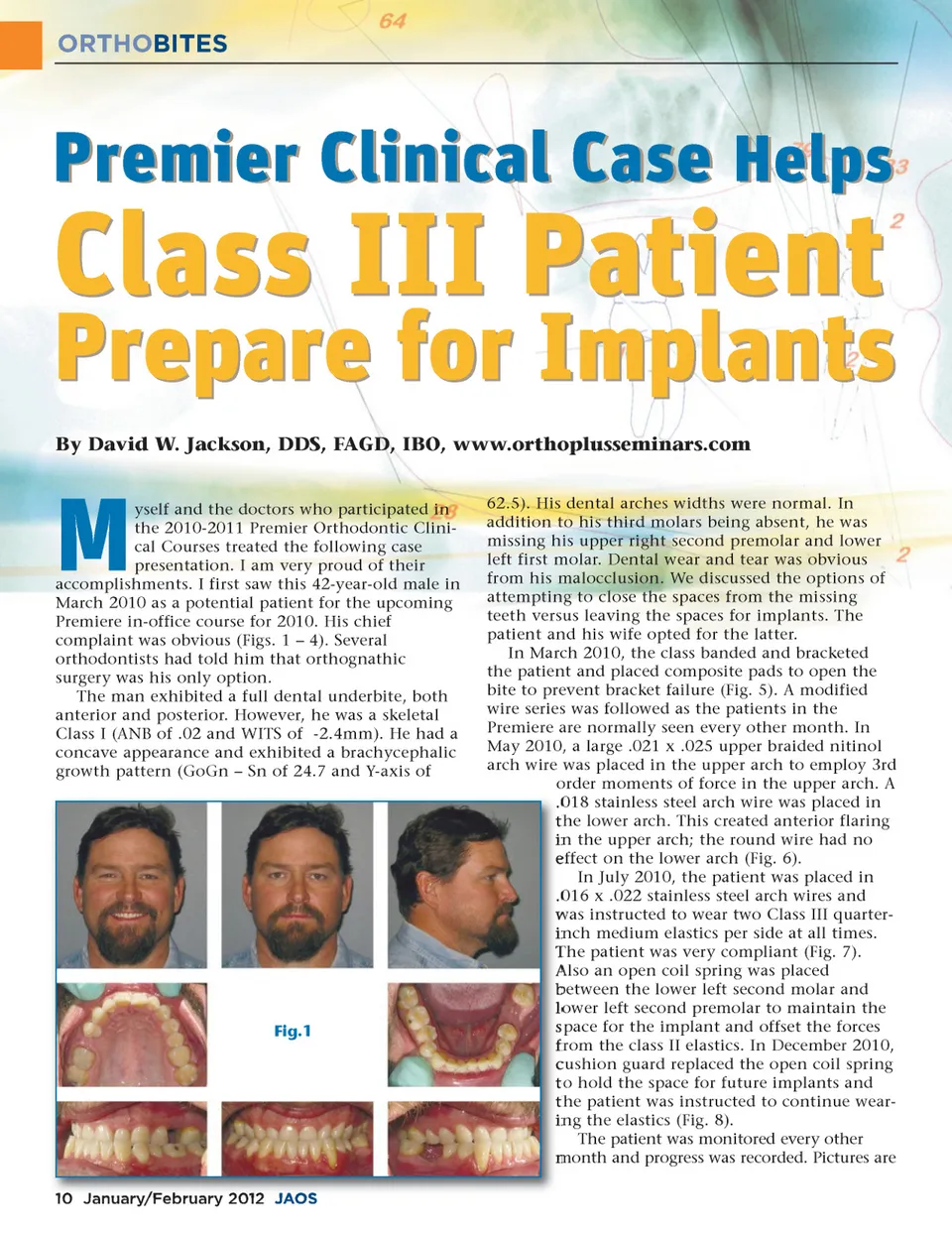
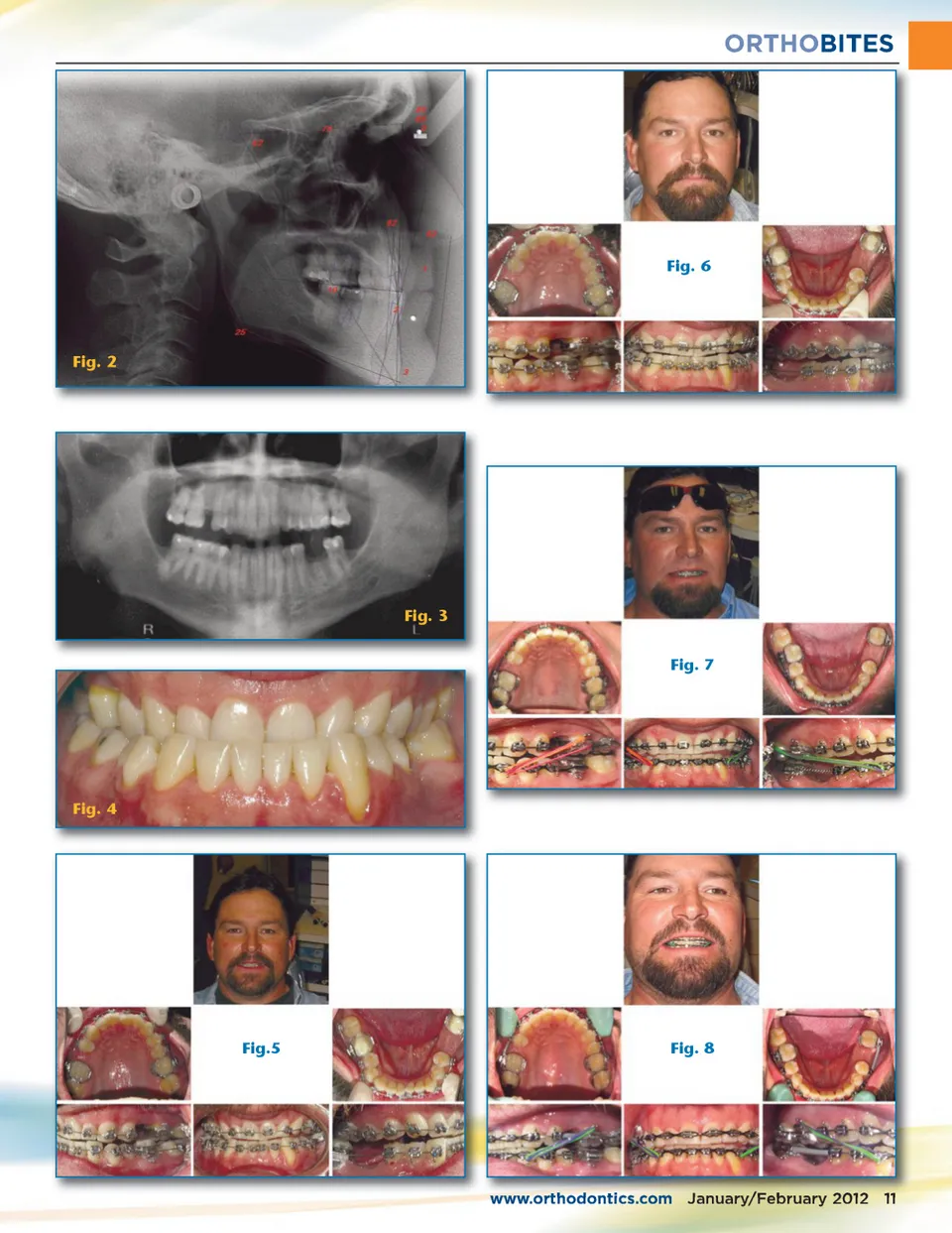
ORTHOBITES Premier Clinical Case Helps Class III Patient By David W. Jackson, DDS, FAGD, IBO, www.orthoplusseminars.com Prepare for Implants M yself and the doctors who participated in the 2010-2011 Premier Orthodontic Clini-cal Courses treated the following case presentation. I am very proud of their accomplishments. I first saw this 42-year-old male in March 2010 as a potential patient for the upcoming Premiere in-office course for 2010. His chief complaint was obvious (Figs. 1 – 4). Several orthodontists had told him that orthognathic surgery was his only option. The man exhibited a full dental underbite, both anterior and posterior. However, he was a skeletal Class I (ANB of .02 and WITS of -2.4mm). He had a concave appearance and exhibited a brachycephalic growth pattern (GoGn – Sn of 24.7 and Y-axis of Fig.1 62.5). His dental arches widths were normal. In addition to his third molars being absent, he was missing his upper right second premolar and lower left first molar. Dental wear and tear was obvious from his malocclusion. We discussed the options of attempting to close the spaces from the missing teeth versus leaving the spaces for implants. The patient and his wife opted for the latter. In March 2010, the class banded and bracketed the patient and placed composite pads to open the bite to prevent bracket failure (Fig. 5). A modified wire series was followed as the patients in the Premiere are normally seen every other month. In May 2010, a large .021 x .025 upper braided nitinol arch wire was placed in the upper arch to employ 3rd order moments of force in the upper arch. A .018 stainless steel arch wire was placed in the lower arch. This created anterior flaring in the upper arch; the round wire had no effect on the lower arch (Fig. 6). In July 2010, the patient was placed in .016 x .022 stainless steel arch wires and was instructed to wear two Class III quarter-inch medium elastics per side at all times. The patient was very compliant (Fig. 7). Also an open coil spring was placed between the lower left second molar and lower left second premolar to maintain the space for the implant and offset the forces from the class II elastics. In December 2010, cushion guard replaced the open coil spring to hold the space for future implants and the patient was instructed to continue wear-ing the elastics (Fig. 8). The patient was monitored every other month and progress was recorded. Pictures are 10 January/February 2012 JAOS
Journal of the American Orthodontic Society January-February 2012: Page 10