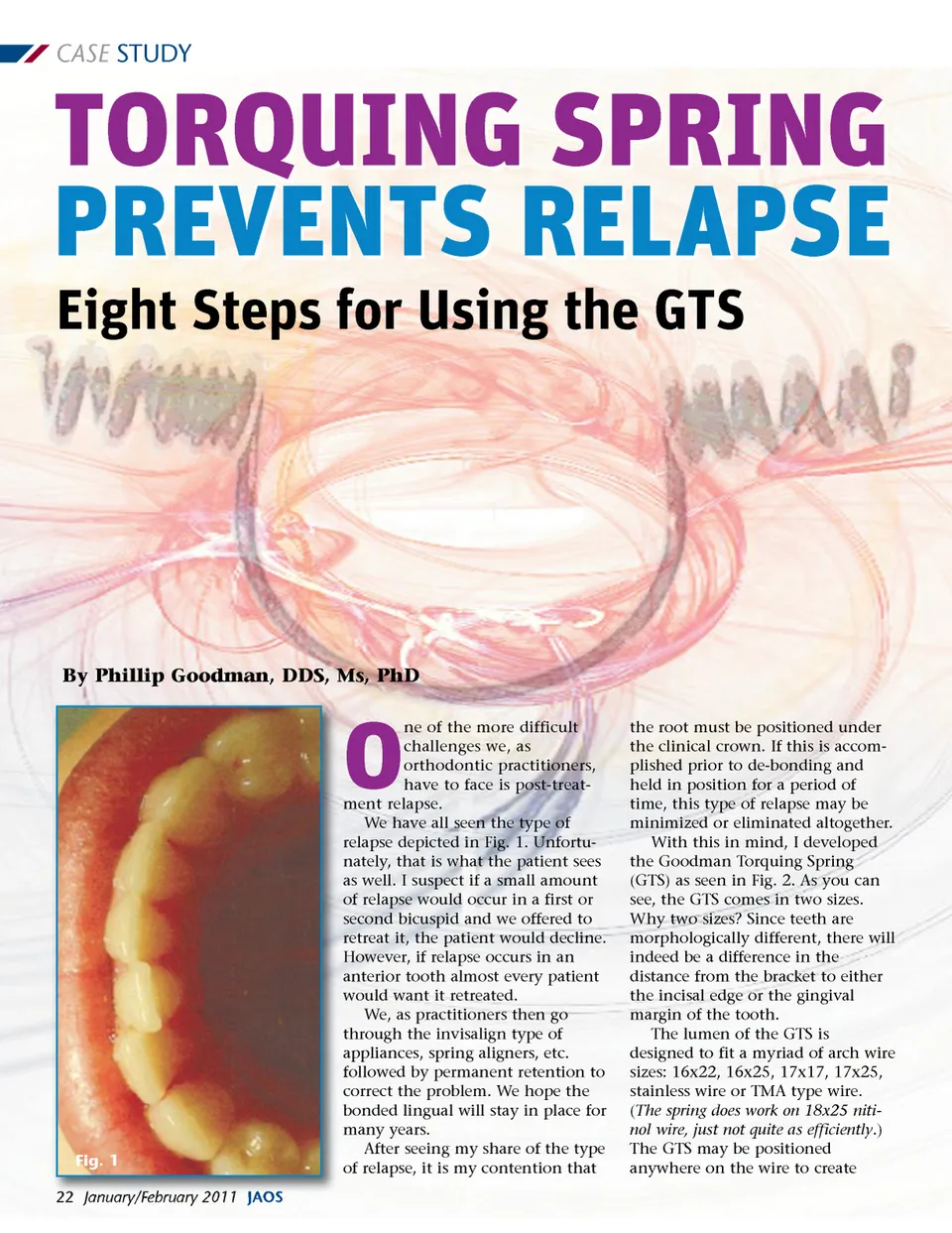
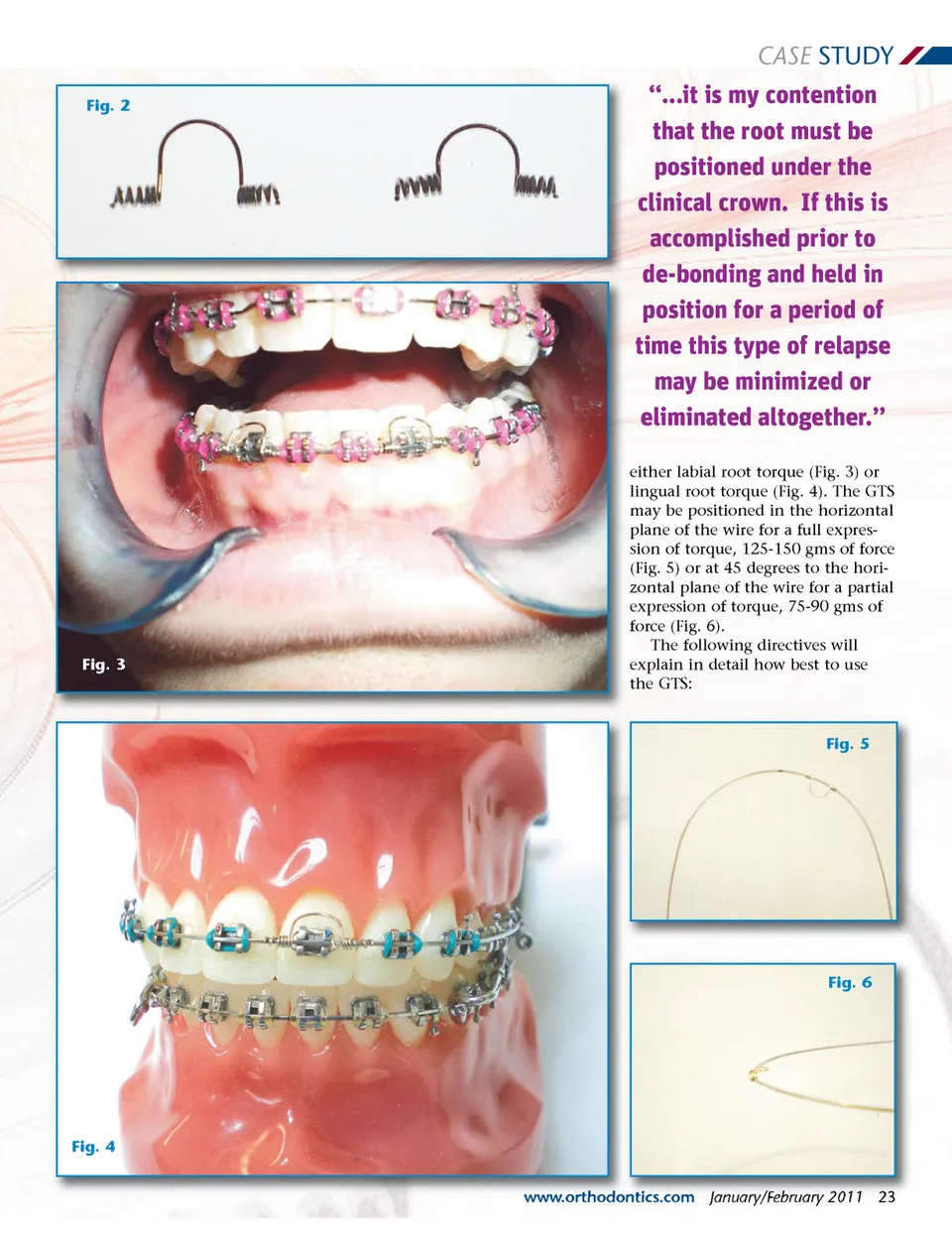
CASE STUDY TORQUING SPRING PREVENTS RELAPSE Eight Steps for Using the GTS By Phillip Goodman, DDS, Ms, PhD O Fig. 1 22 January/February 2011 JAOS ne of the more difficult challenges we, as orthodontic practitioners, have to face is post-treat-ment relapse. We have all seen the type of relapse depicted in Fig. 1. Unfortu-nately, that is what the patient sees as well. I suspect if a small amount of relapse would occur in a first or second bicuspid and we offered to retreat it, the patient would decline. However, if relapse occurs in an anterior tooth almost every patient would want it retreated. We, as practitioners then go through the invisalign type of appliances, spring aligners, etc. followed by permanent retention to correct the problem. We hope the bonded lingual will stay in place for many years. After seeing my share of the type of relapse, it is my contention that the root must be positioned under the clinical crown. If this is accom-plished prior to de-bonding and held in position for a period of time, this type of relapse may be minimized or eliminated altogether. With this in mind, I developed the Goodman Torquing Spring (GTS) as seen in Fig. 2. As you can see, the GTS comes in two sizes. Why two sizes? Since teeth are morphologically different, there will indeed be a difference in the distance from the bracket to either the incisal edge or the gingival margin of the tooth. The lumen of the GTS is designed to fit a myriad of arch wire sizes: 16x22, 16x25, 17x17, 17x25, stainless wire or TMA type wire. ( The spring does work on 18x25 niti-nol wire, just not quite as efficiently .) The GTS may be positioned anywhere on the wire to create
Journal of the American Orthodontic Society January - February 2011: Page 22