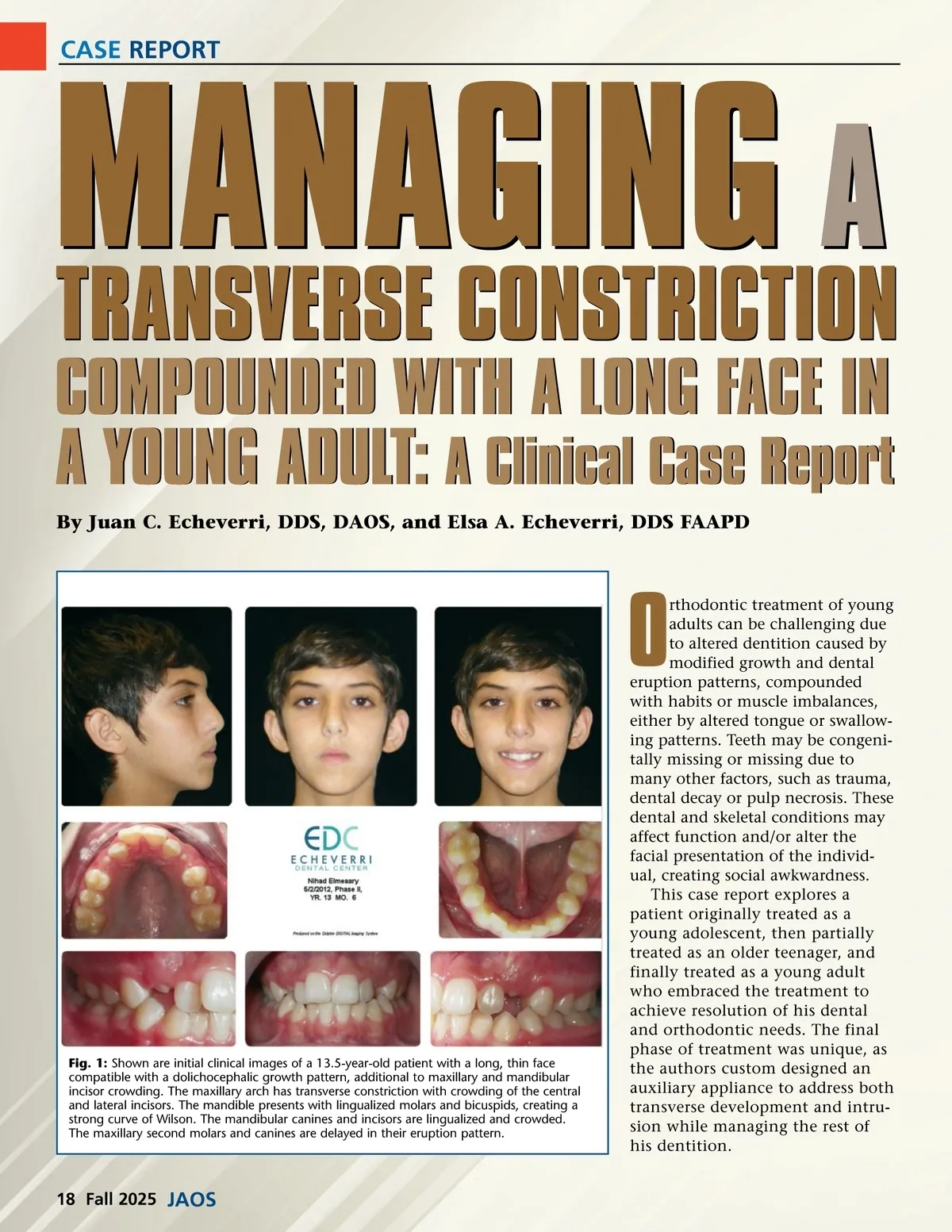
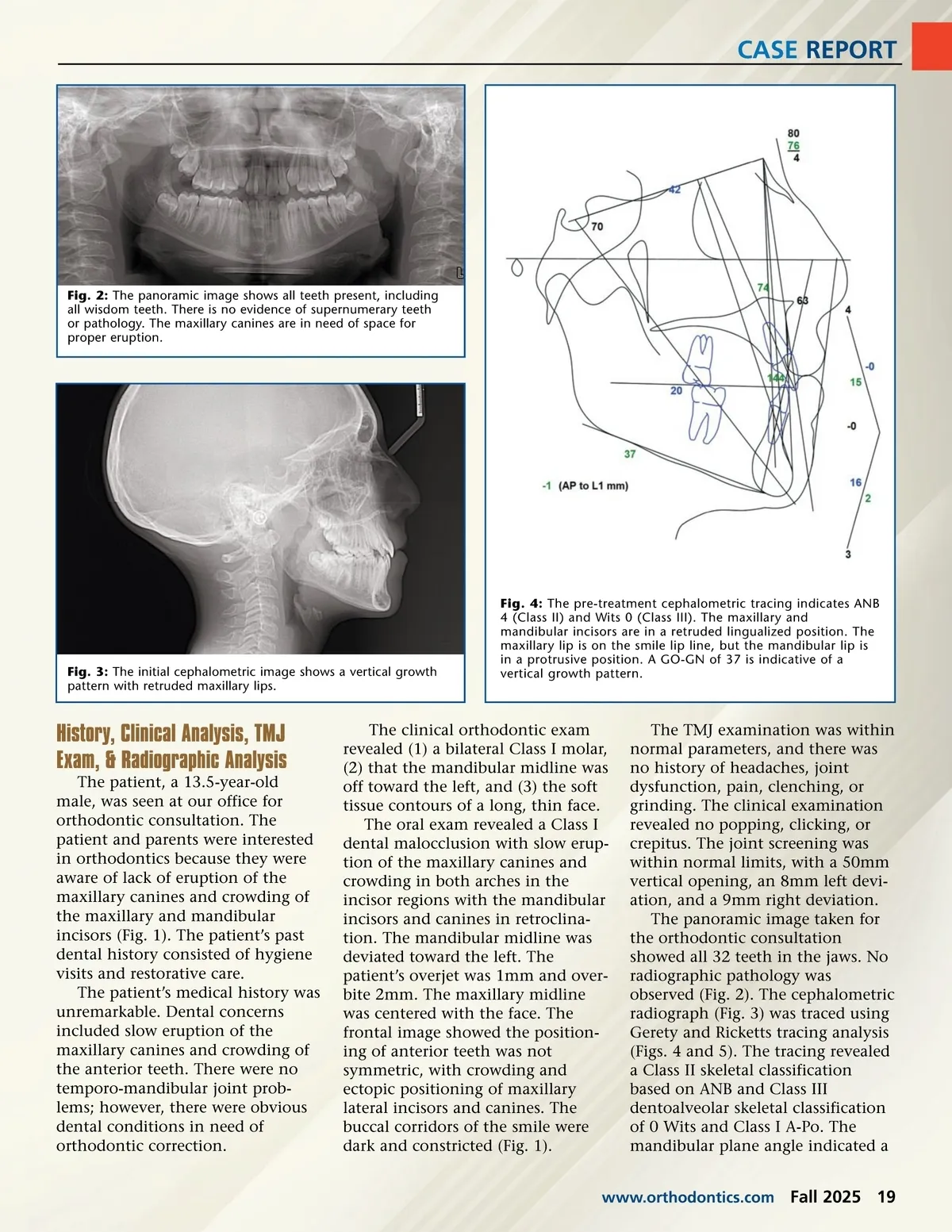
CASE REPORT Fig. 2: The panoramic image shows all teeth present, including all wisdom teeth. There is no evidence of supernumerary teeth or pathology. The maxillary canines are in need of space for proper eruption. Fig. 3: The initial cephalometric image shows a vertical growth pattern with retruded maxillary lips. Fig. 4: The pre-treatment cephalometric tracing indicates ANB 4 (Class II) and Wits 0 (Class III). The maxillary and mandibular incisors are in a retruded lingualized position. The maxillary lip is on the smile lip line, but the mandibular lip is in a protrusive position. A GO-GN of 37 is indicative of a vertical growth pattern. History, Clinical Analysis, TMJ Exam, & Radiographic Analysis The patient, a 13.5-year-old male, was seen at our office for orthodontic consultation. The patient and parents were interested in orthodontics because they were aware of lack of eruption of the maxillary canines and crowding of the maxillary and mandibular incisors (Fig. 1). The patient’s past dental history consisted of hygiene visits and restorative care. The patient’s medical history was unremarkable. Dental concerns included slow eruption of the maxillary canines and crowding of the anterior teeth. There were no temporo-mandibular joint prob-lems; however, there were obvious dental conditions in need of orthodontic correction. The clinical orthodontic exam revealed (1) a bilateral Class I molar, (2) that the mandibular midline was off toward the left, and (3) the soft tissue contours of a long, thin face. The oral exam revealed a Class I dental malocclusion with slow erup-tion of the maxillary canines and crowding in both arches in the incisor regions with the mandibular incisors and canines in retroclina-tion. The mandibular midline was deviated toward the left. The patient’s overjet was 1mm and over-bite 2mm. The maxillary midline was centered with the face. The frontal image showed the position-ing of anterior teeth was not symmetric, with crowding and ectopic positioning of maxillary lateral incisors and canines. The buccal corridors of the smile were dark and constricted (Fig. 1). The TMJ examination was within normal parameters, and there was no history of headaches, joint dysfunction, pain, clenching, or grinding. The clinical examination revealed no popping, clicking, or crepitus. The joint screening was within normal limits, with a 50mm vertical opening, an 8mm left devi-ation, and a 9mm right deviation. The panoramic image taken for the orthodontic consultation showed all 32 teeth in the jaws. No radiographic pathology was observed (Fig. 2). The cephalometric radiograph (Fig. 3) was traced using Gerety and Ricketts tracing analysis (Figs. 4 and 5). The tracing revealed a Class II skeletal classification based on ANB and Class III dentoalveolar skeletal classification of 0 Wits and Class I A-Po. The mandibular plane angle indicated a www.orthodontics.com Fall 2025 19
Journal of the American Orthodontic Society Fall 2025: Page 19