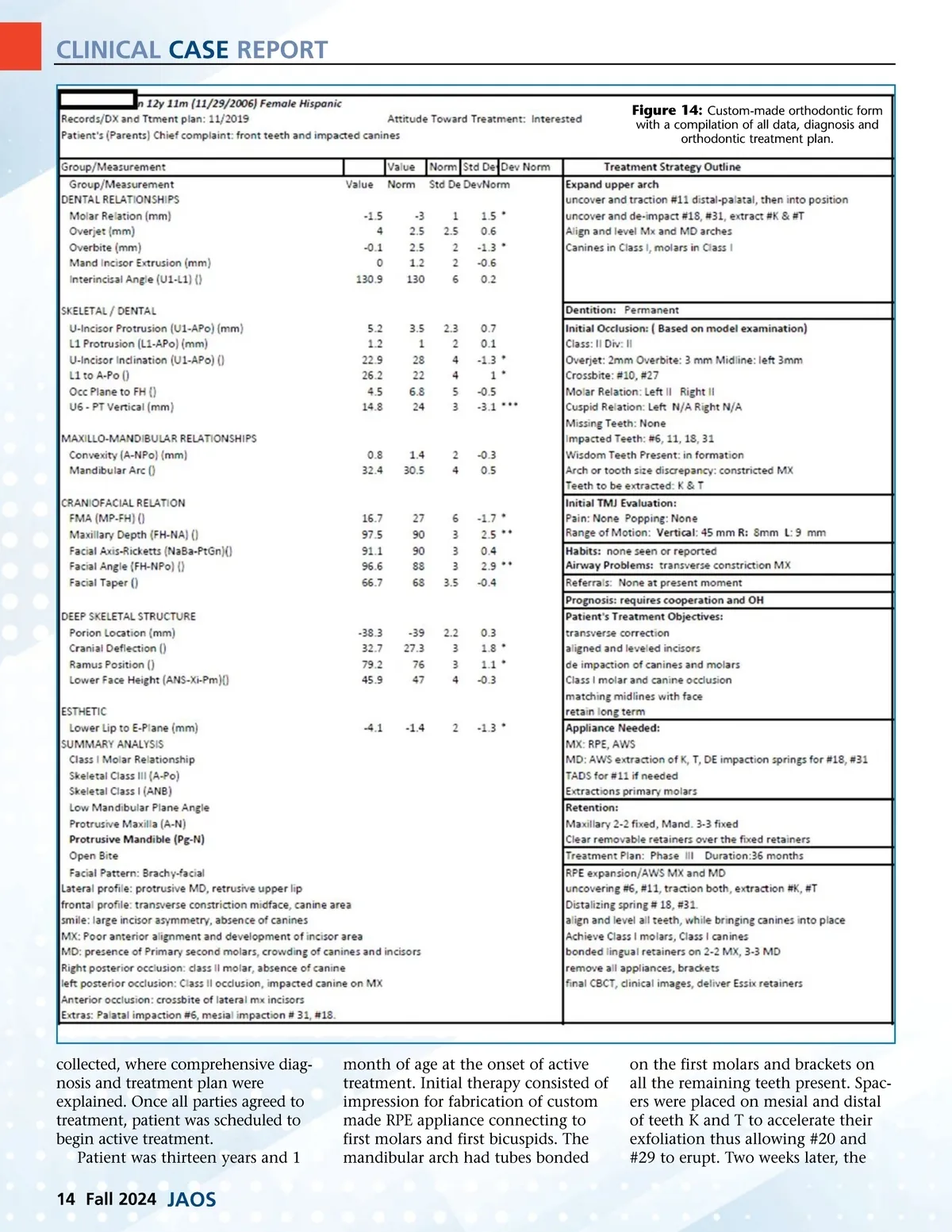
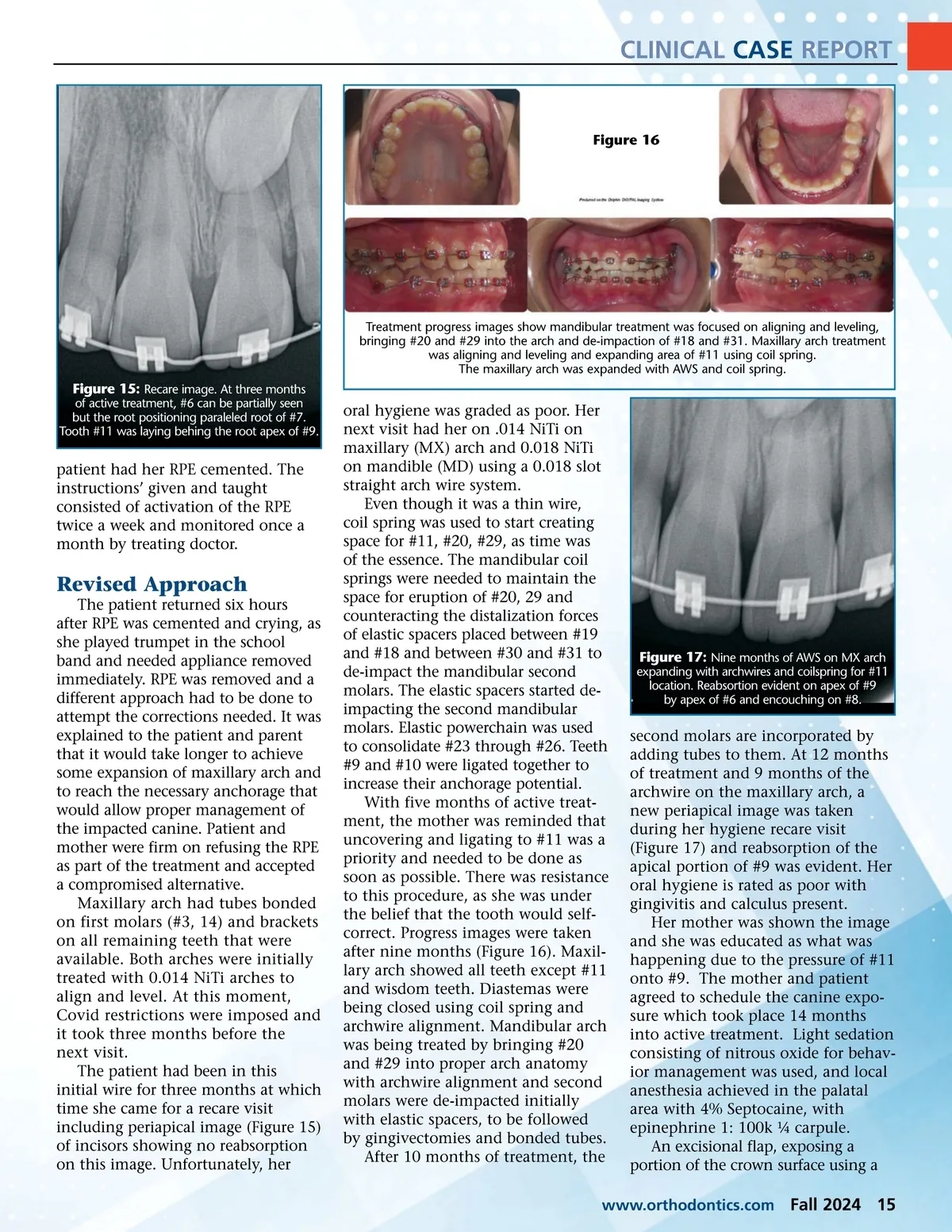
CLINICAL CASE REPORT Figure 16 Treatment progress images show mandibular treatment was focused on aligning and leveling, bringing #20 and #29 into the arch and de-impaction of #18 and #31. Maxillary arch treatment was aligning and leveling and expanding area of #11 using coil spring. The maxillary arch was expanded with AWS and coil spring. Figure 15: Recare image. At three months of active treatment, #6 can be partially seen but the root positioning paraleled root of #7. Tooth #11 was laying behing the root apex of #9. patient had her RPE cemented. The instructions’ given and taught consisted of activation of the RPE twice a week and monitored once a month by treating doctor. Revised Approach The patient returned six hours after RPE was cemented and crying, as she played trumpet in the school band and needed appliance removed immediately. RPE was removed and a different approach had to be done to attempt the corrections needed. It was explained to the patient and parent that it would take longer to achieve some expansion of maxillary arch and to reach the necessary anchorage that would allow proper management of the impacted canine. Patient and mother were firm on refusing the RPE as part of the treatment and accepted a compromised alternative. Maxillary arch had tubes bonded on first molars (#3, 14) and brackets on all remaining teeth that were available. Both arches were initially treated with 0.014 NiTi arches to align and level. At this moment, Covid restrictions were imposed and it took three months before the next visit. The patient had been in this initial wire for three months at which time she came for a recare visit including periapical image (Figure 15) of incisors showing no reabsorption on this image. Unfortunately, her oral hygiene was graded as poor. Her next visit had her on .014 NiTi on maxillary (MX) arch and 0.018 NiTi on mandible (MD) using a 0.018 slot straight arch wire system. Even though it was a thin wire, coil spring was used to start creating space for #11, #20, #29, as time was of the essence. The mandibular coil springs were needed to maintain the space for eruption of #20, 29 and counteracting the distalization forces of elastic spacers placed between #19 and #18 and between #30 and #31 to de-impact the mandibular second molars. The elastic spacers started de-impacting the second mandibular molars. Elastic powerchain was used to consolidate #23 through #26. Teeth #9 and #10 were ligated together to increase their anchorage potential. With five months of active treat-ment, the mother was reminded that uncovering and ligating to #11 was a priority and needed to be done as soon as possible. There was resistance to this procedure, as she was under the belief that the tooth would self-correct. Progress images were taken after nine months (Figure 16). Maxil-lary arch showed all teeth except #11 and wisdom teeth. Diastemas were being closed using coil spring and archwire alignment. Mandibular arch was being treated by bringing #20 and #29 into proper arch anatomy with archwire alignment and second molars were de-impacted initially with elastic spacers, to be followed by gingivectomies and bonded tubes. After 10 months of treatment, the Figure 17: Nine months of AWS on MX arch expanding with archwires and coilspring for #11 location. Reabsortion evident on apex of #9 by apex of #6 and encouching on #8. second molars are incorporated by adding tubes to them. At 12 months of treatment and 9 months of the archwire on the maxillary arch, a new periapical image was taken during her hygiene recare visit (Figure 17) and reabsorption of the apical portion of #9 was evident. Her oral hygiene is rated as poor with gingivitis and calculus present. Her mother was shown the image and she was educated as what was happening due to the pressure of #11 onto #9. The mother and patient agreed to schedule the canine expo-sure which took place 14 months into active treatment. Light sedation consisting of nitrous oxide for behav-ior management was used, and local anesthesia achieved in the palatal area with 4% Septocaine, with epinephrine 1: 100k ¼ carpule. An excisional flap, exposing a portion of the crown surface using a www.orthodontics.com Fall 2024 15
Journal of the American Orthodontic Society Fall 2024: Page 15