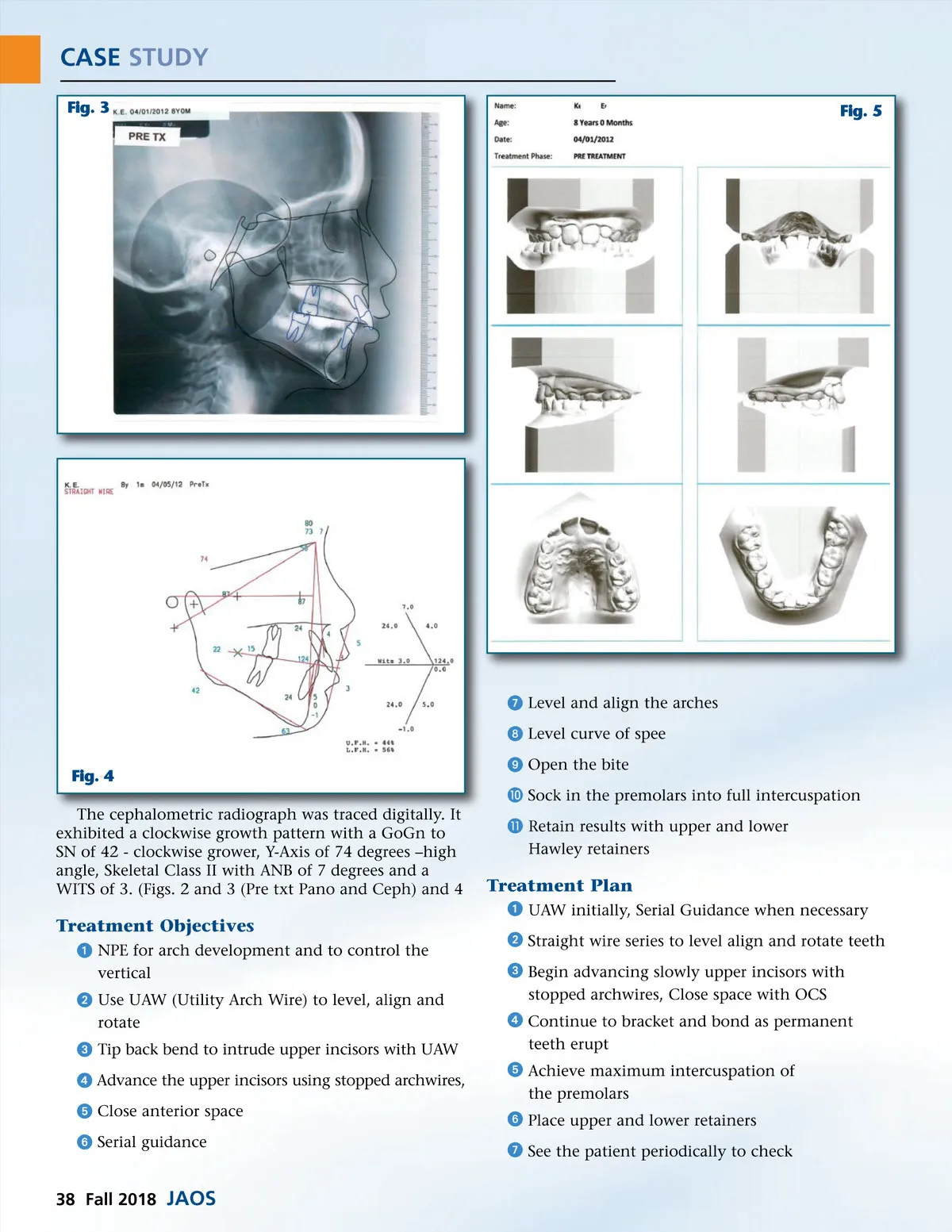
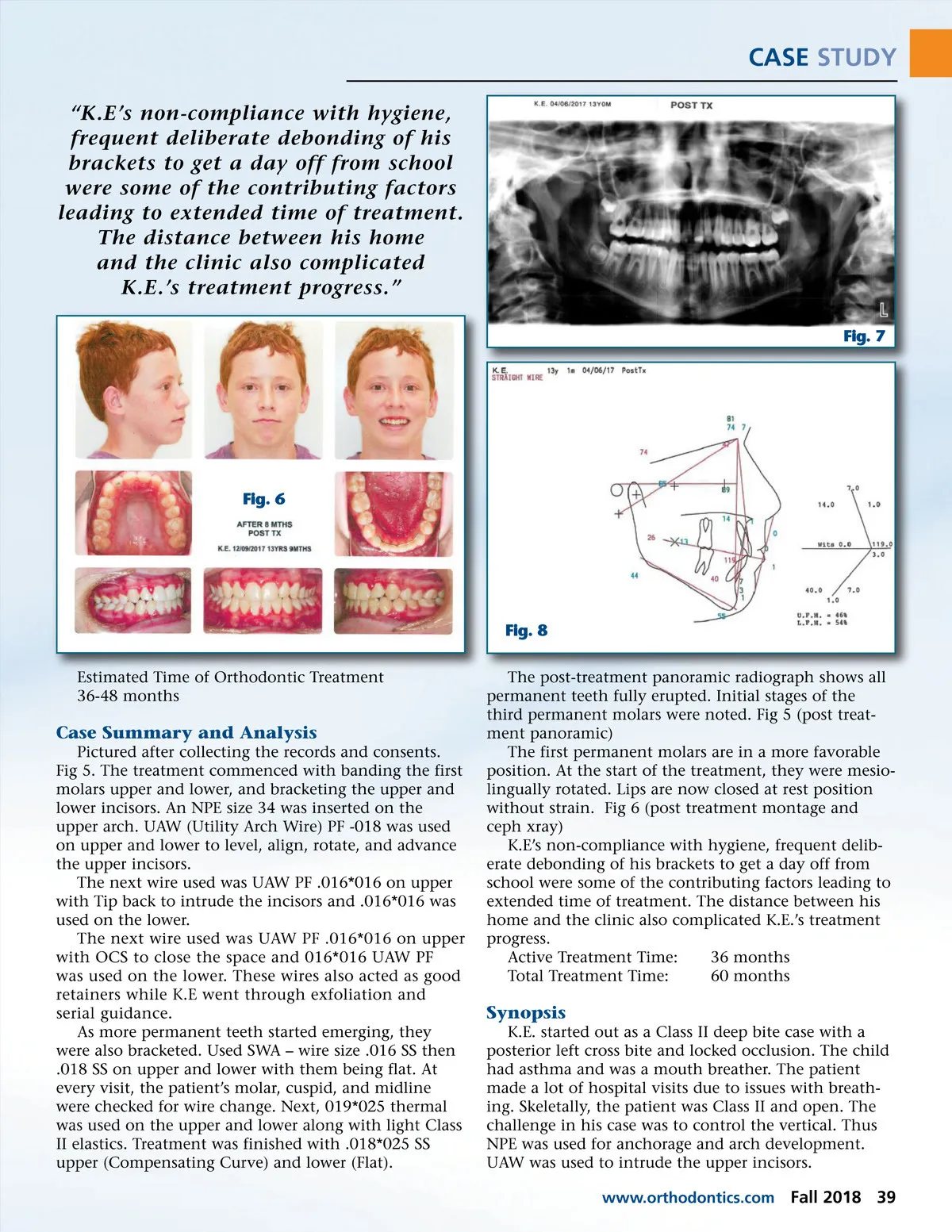
CASE STUDY “K.E’s non-compliance with hygiene, frequent deliberate debonding of his brackets to get a day off from school were some of the contributing factors leading to extended time of treatment. The distance between his home and the clinic also complicated K.E.’s treatment progress.” Fig. 7 Fig. 6 Fig. 8 Estimated Time of Orthodontic Treatment 36-48 months The post-treatment panoramic radiograph shows all permanent teeth fully erupted. Initial stages of the third permanent molars were noted. Fig 5 (post treat-ment panoramic) The first permanent molars are in a more favorable position. At the start of the treatment, they were mesio-lingually rotated. Lips are now closed at rest position without strain. Fig 6 (post treatment montage and ceph xray) K.E’s non-compliance with hygiene, frequent delib-erate debonding of his brackets to get a day off from school were some of the contributing factors leading to extended time of treatment. The distance between his home and the clinic also complicated K.E.’s treatment progress. Active Treatment Time: 36 months Total Treatment Time: 60 months Case Summary and Analysis Pictured after collecting the records and consents. Fig 5. The treatment commenced with banding the first molars upper and lower, and bracketing the upper and lower incisors. An NPE size 34 was inserted on the upper arch. UAW (Utility Arch Wire) PF -018 was used on upper and lower to level, align, rotate, and advance the upper incisors. The next wire used was UAW PF .016*016 on upper with Tip back to intrude the incisors and .016*016 was used on the lower. The next wire used was UAW PF .016*016 on upper with OCS to close the space and 016*016 UAW PF was used on the lower. These wires also acted as good retainers while K.E went through exfoliation and serial guidance. As more permanent teeth started emerging, they were also bracketed. Used SWA – wire size .016 SS then .018 SS on upper and lower with them being flat. At every visit, the patient’s molar, cuspid, and midline were checked for wire change. Next, 019*025 thermal was used on the upper and lower along with light Class II elastics. Treatment was finished with .018*025 SS upper (Compensating Curve) and lower (Flat). Synopsis K.E. started out as a Class II deep bite case with a posterior left cross bite and locked occlusion. The child had asthma and was a mouth breather. The patient made a lot of hospital visits due to issues with breath-ing. Skeletally, the patient was Class II and open. The challenge in his case was to control the vertical. Thus NPE was used for anchorage and arch development. UAW was used to intrude the upper incisors. www.orthodontics.com Fall 2018 39
Journal of the American Orthodontic Society Fall 2018: Page 39