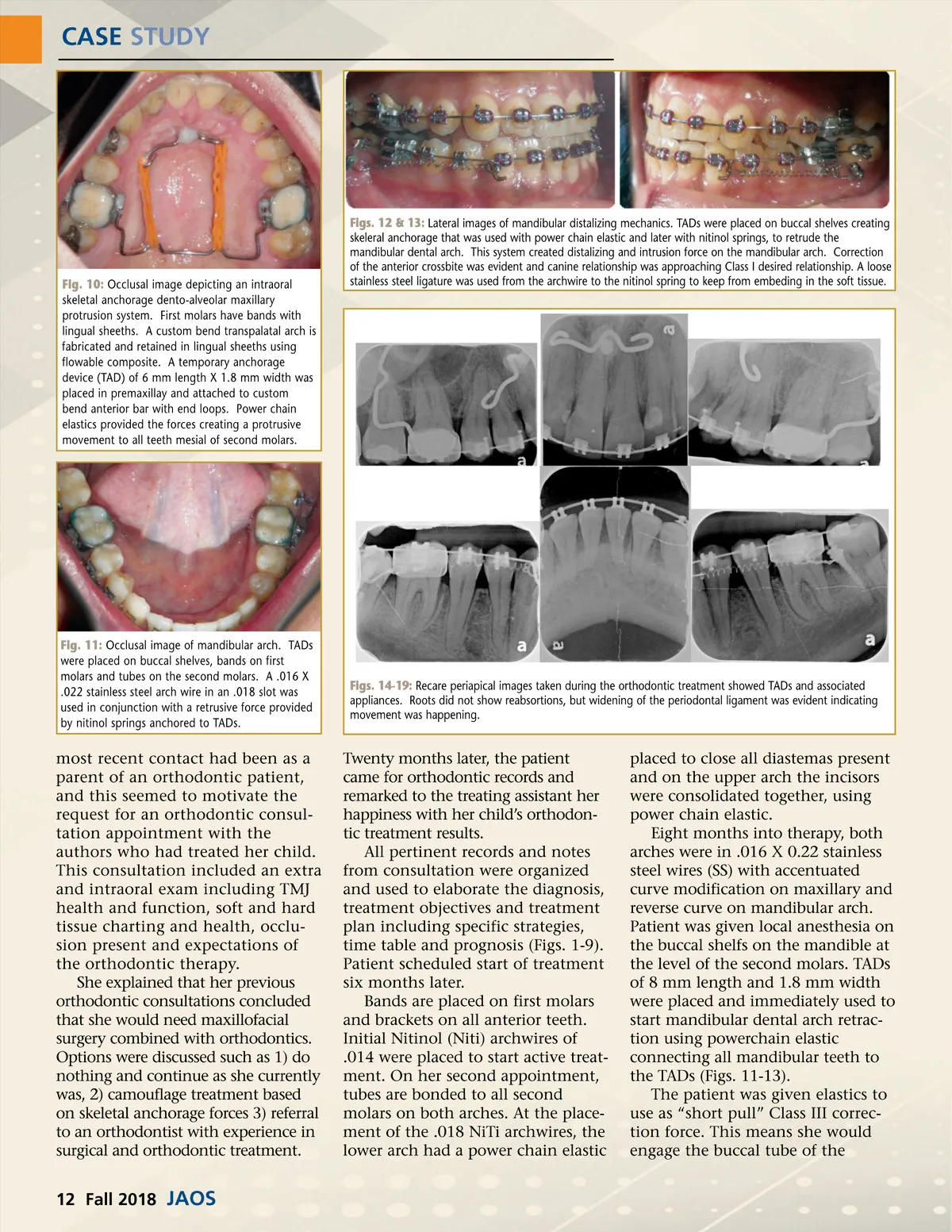
CASE STUDY Fig. 10: Occlusal image depicting an intraoral skeletal anchorage dento-alveolar maxillary protrusion system. First molars have bands with lingual sheeths. A custom bend transpalatal arch is fabricated and retained in lingual sheeths using flowable composite. A temporary anchorage device (TAD) of 6 mm length X 1.8 mm width was placed in premaxillay and attached to custom bend anterior bar with end loops. Power chain elastics provided the forces creating a protrusive movement to all teeth mesial of second molars. Figs. 12 & 13: Lateral images of mandibular distalizing mechanics. TADs were placed on buccal shelves creating skeleral anchorage that was used with power chain elastic and later with nitinol springs, to retrude the mandibular dental arch. This system created distalizing and intrusion force on the mandibular arch. Correction of the anterior crossbite was evident and canine relationship was approaching Class I desired relationship. A loose stainless steel ligature was used from the archwire to the nitinol spring to keep from embeding in the soft tissue. Fig. 11: Occlusal image of mandibular arch. TADs were placed on buccal shelves, bands on first molars and tubes on the second molars. A .016 X .022 stainless steel arch wire in an .018 slot was used in conjunction with a retrusive force provided by nitinol springs anchored to TADs. Figs. 14-19: Recare periapical images taken during the orthodontic treatment showed TADs and associated appliances. Roots did not show reabsortions, but widening of the periodontal ligament was evident indicating movement was happening. most recent contact had been as a parent of an orthodontic patient, and this seemed to motivate the request for an orthodontic consul-tation appointment with the authors who had treated her child. This consultation included an extra and intraoral exam including TMJ health and function, soft and hard tissue charting and health, occlu-sion present and expectations of the orthodontic therapy. She explained that her previous orthodontic consultations concluded that she would need maxillofacial surgery combined with orthodontics. Options were discussed such as 1) do nothing and continue as she currently was, 2) camouflage treatment based on skeletal anchorage forces 3) referral to an orthodontist with experience in surgical and orthodontic treatment. Twenty months later, the patient came for orthodontic records and remarked to the treating assistant her happiness with her child’s orthodon-tic treatment results. All pertinent records and notes from consultation were organized and used to elaborate the diagnosis, treatment objectives and treatment plan including specific strategies, time table and prognosis (Figs. 1-9). Patient scheduled start of treatment six months later. Bands are placed on first molars and brackets on all anterior teeth. Initial Nitinol (Niti) archwires of .014 were placed to start active treat-ment. On her second appointment, tubes are bonded to all second molars on both arches. At the place-ment of the .018 NiTi archwires, the lower arch had a power chain elastic placed to close all diastemas present and on the upper arch the incisors were consolidated together, using power chain elastic. Eight months into therapy, both arches were in .016 X 0.22 stainless steel wires (SS) with accentuated curve modification on maxillary and reverse curve on mandibular arch. Patient was given local anesthesia on the buccal shelfs on the mandible at the level of the second molars. TADs of 8 mm length and 1.8 mm width were placed and immediately used to start mandibular dental arch retrac-tion using powerchain elastic connecting all mandibular teeth to the TADs (Figs. 11-13). The patient was given elastics to use as “short pull” Class III correc-tion force. This means she would engage the buccal tube of the 12 Fall 2018 JAOS
Journal of the American Orthodontic Society Fall 2018: Page 12